Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Benzodiazepine and cyclopyrrolone reduction in general practice — does this lead to concomitant change in the use of antipsychotics?
Journal of Affective Disorders 126 (2010) 293–298
Contents lists available at
Journal of Affective Disorders
Benzodiazepine and cyclopyrrolone reduction in general practice — Doesthis lead to concomitant change in the use of antipsychotics?A study based on a Danish population
Viggo Rask Kragh Jørgensen
Medicine Team, Central Denmark Region, Lægårdvej 12, 7500 Holstebro, Denmark
Introduction: In the period 2004–2006, 15 doctors in the Danish municipality of Lemvig
Received 11 February 2010
introduced a more restrictive approach to the prescription of benzodiazepines and
Received in revised form 6 March 2010
cyclopyrrolones. A prescription could be renewed only following personal consultation, and
Accepted 7 March 2010Available online 22 April 2010
prescriptions were issued for only a single month's usage. The intervention reduced theprescription of benzodiazepine anxiolytics by 50%, cyclopyrrolones by 57% and benzodiazepinehypnotics by 55% over a 1½ year period. There is a paucity of knowledge about whether such an
intervention reduces drug consumption in general or merely shifts consumption to other
drugs. Here especially antipsychotics (AP) are in the spotlight.
Materials and methods: The current article describes the prescription of antipsychotics before
and after the intervention. Consumption was followed via the Danish Medicines Agency's
website Ordiprax, where the quantity of pharmacy-sold prescription drugs by individual
medical practices can be monitored.
Results: The overall increase in the prescription of antipsychotics during the interventiondescribed here was not more than 3.1% of the reduction in prescriptions of benzodiazepine andcyclopyrrolone measured in defined daily doses (DDD).
Conclusion: The intervention against benzodiazepine and cyclopyrrolone did not result in anuncontrollable increase in the prescription of antipsychotic drugs. It cannot be excluded thatthe intervention impacted individual prescriptions. For future interventions of a similar nature,it is recommended that GPs are trained in the use of antipsychotics.
2010 Elsevier B.V. All rights reserved.
Benzodiazepines were introduced in 1960 as a successor
Their hypnotic effect disappears
to the barbiturates, chloral hydrate and meprobamate
after a few months, while their anxiolytic effect has almost
Specific advantages include their
disappeared after a few months (
low toxicity and broad therapeutic application. It is now
). Accordingly, patients are consuming
recognized that there are significant problems associated
medicines which have no positive effect in long-term
with the use of benzodiazepines and cyclopyrrolones. They
may give rise to strong dependence with a pronounced
In Denmark 8.2% of the population were users of
tolerance development
benzodiazepines and cyclopyrrolones in 2008 ). The problem is not only Danish, and the number ofusers in, for example, Ireland and Spain is 25% and 18% of thepopulation respectively. In Norway the corresponding figureis 6.5% of the adult population ). In
⁎ Ærøvej 1b, 7680 Thyborøn, Denmark. Tel.: +45 97 832300 (Work), +45
Denmark it is estimated that around 2% of the population is
97 832493 (Private); fax: + 45 97 832057.
dependent on these substances (
0165-0327/$ – see front matter 2010 Elsevier B.V. All rights reserved.
V.R.K. Jørgensen / Journal of Affective Disorders 126 (2010) 293–298
1. Materials and methods
corresponding figure for Switzerland is 1.6% ).
Data were obtained from 15 general practitioners,
The rules for the prescription of benzodiazepines and
covering 12 medical practices in the Danish municipality of
cyclopyrrolones are almost identical in, for example, England,
Lemvig. Doctors had a patient base of approximately 20,830
Norway and Denmark
patients, of which approximately 1000 patients participated
Benzodiazepines and cyclopyrrolones should only be pre-
in the intervention All practices
scribed for a few weeks, after which a re-evaluation must take
participated in the intervention against the overuse of
place. These rules of good clinical practice were first
benzodiazepines and cyclopyrrolones. The two primary
advocated in 1988 in a Bulletin of the Royal College of
practices initiated the intervention in 2004 and the remaining
Psychiatrists (However, no
10 practices followed after the second quarter of 2005. The
methods for implementation where indicated, and the
practices' results are calculated as the average quarterly
scientific basis for the effectiveness of these rules was
prescription in the years preceding the intervention, followed
by prescription six quarters later.
In 2003, doctors at two medical practices in the Danish
The data compiled here are grouped according to their
village of Thyborøn chose to address the issues
Anatomical Therapeutic Chemical (ATC) codes The
groups give a complete overview of antipsychotics registered
collaboration with the Medicine Unit of Ringkjøbing County
in Denmark, and are included for the sake of completeness,
and the County Medical Health Officer, a few simple rules
without considering their direct relevance and usefulness as
were introduced in the two practices for the prescription of
substitutes for benzodiazepines and cyclopyrrolones.
benzodiazepines and cyclopyrrolones, including:
The internet site was used for
evaluation ), since data were easily
available and covers the desired material.
the discontinuation of telephone prescriptions
The Ordiprax data base comprises data reported by
prescription only following personal consultation
pharmacists to the Danish Medicines Agency Pharmaceutical
prescription for a maximum of 1 month's consumption
Statistics Register for the sale of prescription drugs toindividuals, registered as number of defined daily doses
The intervention led to the patient and the doctor re-
evaluating on a monthly basis whether current prescription
The average of the prescribed volume of antipsychotics
levels were appropriate and therefore should continue, or
in the four quarters preceding the intervention, is termed
whether a reduction should be initiated.
pre-intervention ("Before"). In practices 1 and 2, "Before"
In a 3 1/4 year period from 2004, the two practices achieved
data covers the year 2003, and for the other practices the
a significant reduction in the prescription of benzodiazepine
period from the second quarter of 2004 to first quarter of
anxiolytics by 85%, of cyclopyrrolones by 91% and of benzodi-
2005. The average of the prescribed volume of antipsycho-
azepine hypnotics by 83% . The remain-
tics six quarters after the initiation of the intervention is
ing doctors in the municipality were inspired, and subsequently
termed post-intervention ("After"). In practices 1 and 2 this
introduced similar rules in their practices. One and a half
covers the second quarter of 2005, and the third quarter of
years after the joint implementation of the rules, prescrip-
2006 for the other practices. The total prescribed volume as
tions of benzodiazepine anxiolytics were reduced by 50%,
well as the prescribed volume of all of the subgroups was
cyclopyrrolones by 57% and benzodiazepine-hypnotics by
55% (). The overall reduction of benzo-
In order to facilitate comparison with data from the rest of
diazepines and cyclopyrrolones was 2395 DDD / 1000 patients
the country, gender and age-standardized data were chosen
and no specific information on antipsychotics was given to
Among colleagues it was argued that consumption was
patients, or to the staff of the participating physicians, and no
probably just transferred to antipsychotics instead. This
unusual prescription initiatives in this area were implemented.
objection is academically relevant, as it is known that other
The annual average increase in the prescription of
interventions of a similar nature have lead to a shift in the
antipsychotics for the county was calculated on the basis of
consumption of other drugs (). The use
quarterly figures from 2003 to 2006. County prescription
of antipsychotics for anxiety disorders are generally consid-
levels are illustrated through the use of a bar chart with error
ered to be scientifically poorly elucidated (
bars indicating the least significant difference (LSD), p = 0.05
). In Denmark antipsychotics have occasionally been
calculated using analysis of variance (ANOVA) followed by
used for the treatment of anxiety disorders.
the Student–Newman–Keuls post-ANOVA test.
This article seeks to illuminate the issue of whether an
intervention as described above leads to an actual reduction
in benzodiazepine and cyclopyrrolone consumption ormerely shifts consumption to other drugs, and the article
2.1. County results
focuses on changes in the prescription of antipsychoticsfollowing a systematic review of the group. The article also
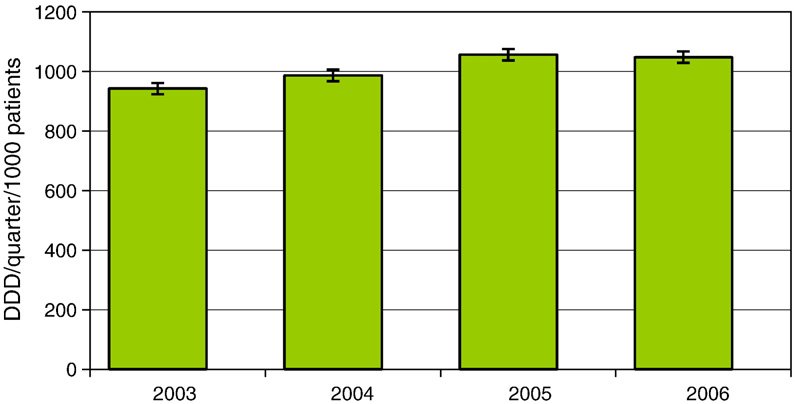
The county prescription of antipsychotics increased by
aims to strengthen the basis for decision-makers in health
3.7% per year on average during the period 2003–6. The
systems who work with addictive medication, as well as
increase was statistically significant (see ). At the
being an inspiration to fellow practitioners.
national level, the increase during the period 2005–6 was 2%.
V.R.K. Jørgensen / Journal of Affective Disorders 126 (2010) 293–298
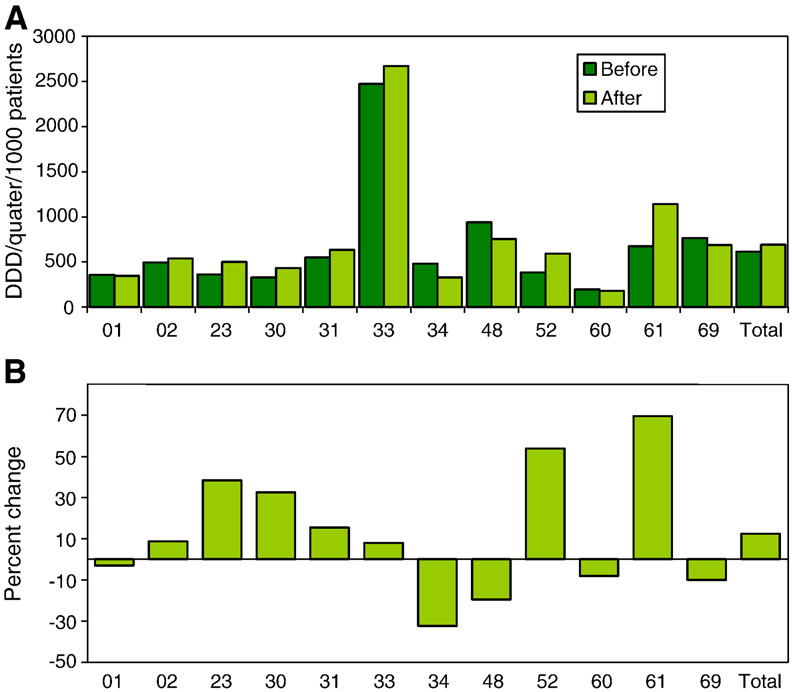
Each practice had differences in the prescription of
The classification of antipsychotics after the Anatomical Therapeutic Chemical
antipsychotics ranging from 194 to 2474 DDD/1000 patients
Classification System (ATC)-codes.
per quarter at initiation of the intervention. Six quarters after
the initiation the differences ranged from 178 to 2669 DDD/
1000 patients per quarter. There were also considerable
differences in the percentage change in prescriptions, theseranged from a decline of 32% to an increase of 70%. Practice 33
was assigned to the area's only psychiatric institution
Phenothiazines with aliphatic side chains
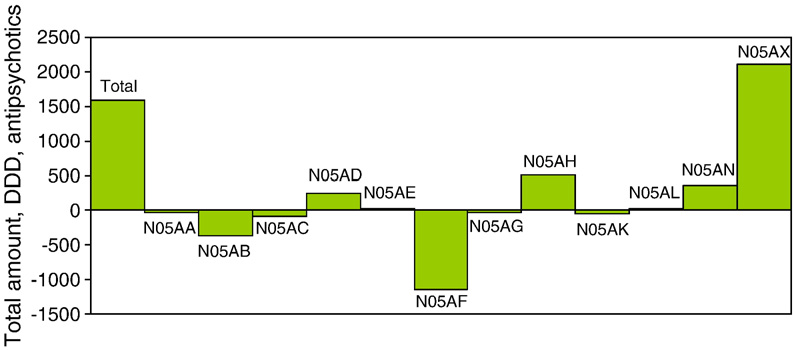
The changes in prescriptions within the individual sub-
groups are shown in During the initiative the groups
N05AF and N05AX showed marked changes. The other groups
had only minor variations in prescriptions.
Phenothiazines with piperazine structure
In the group N05AF prescription decreased by 37%,
equivalent to 1151 DDD throughout the municipality,
corresponding to 55 DDD per 1000 patients. This group
first generation antipsychotics. At the national
Phenothiazines with piperidine structure
level, prescription in this group is also declining.
Group N05AX consists of second generation antipsycho-
tics and shows a numerical increase of 2105 DDD throughout
the municipality, representing an increase of 167%. The
corresponding result is 101 DDD/ 1000 patients per quarter.
At the national level, a marked increase in prescription also
took place within this group.
N05AEIndole derivatives
A Danish study from 2003 reveals that 12% of patients
Thioxanthen derivatives
undergoing a reduction in their prescriptions of benzodiaz-
epine were prescribed an alternative nerve medicine,
including a signi
ficant proportion of antipsychotics (
The overall municipal increase in the prescription of
antipsychotics during the intervention was 12.4%, represent-
ing an annual increase of 8.2%. The corresponding numerical
N05AHDiazepins and oxazepines
increase was 76 DDD/1000 patients per quarter. This is
considerably larger than the statistically significant increase
at the county level of 3.7% per year during the intervention
period. However this amount corresponds to less than one
patient having been treated with 1 DDD/1000 patients per
Neuroleptica for tardive dyskinesia
quarter. This should also be compared to the fact that the
overall reduction in the prescription of benzodiazepines and
cyclopyrrolones was 2395 DDD/1000 patients per quarter
). Thus, the increase in prescription of
antipsychotics was merely 3.1% of the reduction in prescrip-
tions of benzodiazepines and cyclopyrrolones measured in
This increase in the prescription of antipsychotics is
Other antipsychotics
mainly ascribed to the N05AX group, comprising Risperidone
(risperdal, ridal) and Aripiprazole (abilify). Both are secondgeneration antipsychotics and are generally regarded to be atleast as effective as first generation antipsychotics, and are
2.2. Municipality results
much better tolerated with fewer side effects. This group isincreasingly prescribed by local psychiatrists. The N05AF
In Lemvig municipality the average prescription of
group comprising Flupentixol (fluanxol, depixol, emergil)
antipsychotics in 2003 was 65% of county prescription levels
Chlorprothixene (truxal, taractan) and Zuclopenthixol (cisor-
at initiation of the intervention.
dinol, clopixol, acuphase) are first generation antipsychotics,
The overall increase in the prescription of antipsychotics
and their use is decreasing. This is consistent with the general
during the intervention was 12.4%, which represents an
national trend ), which is to replace the
annual increase of 8.2%. The numerical increase was 76 DDD/
older first generation antipsychotics with more modern,
1000 patients per quarter, representing an annual increase of
second generation antipsychotics having fewer side effects.
51 DDD/1000 patients per quarter.
The prescription of Flupentixol is declining in spite of the fact
V.R.K. Jørgensen / Journal of Affective Disorders 126 (2010) 293–298
Fig. 1. The total volume of prescribed antipsychotics in Ringkøbing County. The columns indicate average daily defined doses (DDD) per quarter per thousandregistered patients for the year indicated. Errors bars indicate least significant difference (p = 0.05) calculated using Analysis of Variance followed by the Student–Newman–Keuls post-ANOVA test.
that is has, to some extent, been prescribed for anxiety
increase in prescription of antipsychotics noted in the
disorders. The N05AF group is mostly prescribed by psychia-
municipality during the intervention may be attributed to
trists, and general practices are usually responsible for
patients with psychiatric diseases for whom, upon reduction
prescription renewals. For the remaining groups of antipsy-
of their prescriptions of benzodiazepine and cyclopyrrolone,
chotics, changes in prescription volumes are so small that
it is discovered that they could be more appropriately treated
they are judged to be irrelevant to this study as prescriptions
for a few patients could influence the results.
In accordance with the present study, the consumption of
In Lemvig municipality the prescription of antipsychotics
antidepressants during the intervention showed no signifi-
is substantially under the county average. Part of the
cant increase ).
explanation may be that there is only one major psychiatric
This study does not address the quality of treatment with
institution in the area. There may therefore be a departure
antipsychotics. It is also not possible to infer from the results
from the municipality by users of antipsychotics to regions
whether an under- or over-treatment took place. In addition,
having multiple psychiatric facilities. Part of the slight
the study provides no information about changes in prescrip-
Fig. 2. Change in the prescription of antipsychotics for individual practices over a 1½ year period. On the x-axis, practices are identified by a double-digit code, with"Total" Indicating the total average change. (A) Changes in the daily defined doses (DDD) per quarter per thousand registered patients. The first column indicatesthe average prescription rate in the four quarters prior to the intervention ("Before"), while the second column indicates the prescription rate in the sixth quarterfollowing the start of the intervention ("After"). (B) The percent change in prescriptions of antipsychotics for individual practices.
V.R.K. Jørgensen / Journal of Affective Disorders 126 (2010) 293–298
Fig. 3. Change in the total prescription of antipsychotics issued by twelve Danish practices, during six quarters following the start of the intervention. The firstcolumn ("Total") indicates the total change in prescriptions. On the x-axis antipsychotic groups are identified as defined in
tions to individual users or about changes in the numbers of
users. This study answers only the question of whether thetotal prescribed amount of antipsychotics increased as a
Thanks are extended to practitioners in Lemvig for their
result of the restrictive attitude towards the prescription of
cooperation, as well as their willingness to be the first to
benzodiazepines and cyclopyrrolones.
implement the new rules in a larger region.
The intervention was implemented on a voluntary basis in
Lemvig. The patient was at all times the focal point of the
intervention, and changes in prescriptions were the result ofmonths of consultations and were usually based on
Anonymous, 1980. Systematic review of the benzodiazepines. Guidelines for
data sheets on diazepam, chlordiazepoxide, medazepam, clorazepate,lorazepam, oxazepam, temazepam, triazolam, nitrazepam and fluraze-
The overall result shows that a reduction in the prescrip-
pam. Committee on the Review of Medicines. BMJ 280 (6218), 910–912
tion of benzodiazepines and cyclopyrrolones does not
necessarily lead to a concomitant, uncontrollable increase in
Anonymous. Helsetilsynet. Vanedannende legemidler. Forskrivning og
forsvarlighet. 14. september 2001. [in Norwegian]
the prescription of psychotherapeutic drugs. In the individual
[Accessed 2009 Okt 15].
practices involved in the intervention, a considerable varia-
Anonymous. Benzodiazepines warning, Chief Medical Officer's Update 37,
tion in changes in the prescription of antipsychotics could be
Patient Safety, Department of Health, 2004. [Accessed 2009 Oct 15].
observed. Accordingly, the education of practitioners in the
Anonymous. Referenceprogram for angstlidelser hos voksne. København:
prescription of alternative psychotherapeutic drugs is to be
Sundhedsstyrelsen, 2007[ In Danish].
recommended in future interventions of a similar nature.
[Accessed 2009 Okt 15].
Anonymous. Communication regarding the prescription of addictive drugs.
Danish National Board of Health. Juli 2008.
[Accessed 2009 Oct 15].
Anonymous. Roche Hjemmeside,
[Accessed 2009 Okt 15] ].
A reduction in the prescription of benzodiazepine and
Anonymous. Ordiprax: a tool for doctors and regions. Fact sheet from the
cyclopyrrolone does not necessarily lead to a concomitant,
Danish Medicines Agency [online]. Available from [Accessed 2009 December 6].
uncontrollable increase in the prescription of antipsychotic
Ashton, C.H., 2002. Benzodiazepines: how they work and how to withdraw.
drugs. The overall increase in the prescription of antipsycho-
The Ashton manual. Aug.,
tics during the intervention described here was not more
[Accessed 2009 Okt 15].
than 3.1% of the reduction in prescriptions of benzodiazepine
Gesser, K. Lægemiddelstyrelsen, Mail of 17. februar 2009 (Personal
and cyclopyrrolone measured in DDD.
Gyldmark, M., Hansen, E.H., 1997. De samfundsmæssige omkostninger ved
It is therefore recommended that the few simple rules
afhængighed af psykofarmaka. Danmarks farmaceutiske Højskole.
presented here are followed when prescribing benzodiaze-
Lægemiddelforskning 36–37 [in Danish][online]. Available from URL:
pines and cyclopyrrolones.
[Accessed 2010 Jan 25].
Hansen, E.H., Helweg-Jørgensen, S., 1999. Afhængighed af psykofarmaka set
fra brugernes side. Faculty of Pharmaceutical Sciences. Lægemiddel-
Role of the funding source
forskning 22–23 [cited: 20th Feb 2010]. Available from:
The author has received honoraria from public funding for the further
education of practitioners for lecturing on drug reduction in clinical practice.
Jørgensen, V.R.K., 2007. An approach to reduce benzodiazepine and
cyclopyrrolone use in general practice, a study based on a danishpopulation. CNS Drugs 21 (11), 947–955.
Conflict of interest
Jørgensen, V.R.K. Can the consumption of benzodiazepines and cyclopyrro-
The author is a part time employee of the Medicine Team, Central
lones be reduced in generel practice? Siicsalud 2009 may,5.
Denmark Region, and has received honoraria from public funding for the
[Accessed 2010 marts 6].
further education of practitioners for lecturing on drug reduction in clinical
Jørgensen, V.R.K., 2010. Benzodiazepine and cyclopyrrolone reduction in
practice, as well as funding within the constraints of the Danish Medicines
general practice — does this lead to change in the use of antidepressants?
Agency from the pharmaceutical industry for three lectures on drug
A study based on a Danish population. J. Affect. Disord. 125 (1–3),
reduction in clinical practice.
V.R.K. Jørgensen / Journal of Affective Disorders 126 (2010) 293–298
Jørgensen, V.R.K., Toft, B.S., 2008. Reduction in the use of benzodiazepines
Priest, R.G., Montgomery, S.A., 1988. Benzodiazepines and dependence: a
and cyclopyrrolones in general practice. Pharm. Pract. 6 (3), 136–141.
college statement. Bull. R. Coll. Psychiatry 12, 107–109.
Jørgensen, V.R.K., Toft, B.S., Fogh, M.S., 2006. Reducing the use of
Srisurapanont, M., Critchley, J., Garner, P., Maneeton, B., Wongpakaran, N.,
benzodiazepines and cyclopyrrolones in clinical practice! [in Danish].
2006. Interventions to reduce benzodiazepine prescribing (Protocol).
Ugeskr Laeger 168, 1636–1640.
Cochrane Database Syst. Rev. (2), CD005172.
Jørgensen, V.R.K., Toft, B.S., Fogh, M.S., 2006. Reducing the use of
The Danish Medicines Agency. Development of benzodiazepine consumption
benzodiazepines and cyclopyrrolones in clinical practices. Pharm.
in Denmark 1996–2003. [online]. Available from URL:
Pract. 4 (2), 74–78.
2010 Jan 21].
Lader, M., 1991. History of benzodiazepine dependence. J. Subst. Abuse Treat.
Weintraub, M., Singh, S., Byrne, L., Maharaj, K., Guttmacher, L., 1991.
8 (1–2), 53–59.
Consequences of the 1989 New York State triplicate benzodiazepine
Petitjean, S., Ladewig, D., Meier, C.R., Amrein, R., Wiesbeck, G.A., 2007.
prescription regulations. JAMA 6 (266(17)), 2392–2397.
Benzodiazepine prescribing to the Swiss population: results from anational survey of community pharmacies. Int. Clin. Psychopharmacol.
22, 292–298.
Source: http://www.cure4you.dk/zendpublic/clinic/1621/file/journal_of_affective_disorders_2.pdf
University Department of Pharmaceutical Sciences Evaluative Report of the Programme Name of the Programme: University Department of Pharmaceutical Sciences Year of establishment : Is the Department part of a School/Faculty of the university? Faculty of Science and Technology Names of programmes offered (UG, PG, M.Phil., Ph.D., Integrated Masters; Integrated Ph.D., D.Sc., D.Litt., etc.) : a. PG - M. Pharm. in six different specializations viz.,
NIH Public AccessAuthor ManuscriptBrain Res. Author manuscript; available in PMC 2013 August 01. NIH-PA Author Manuscript Published in final edited form as: Brain Res. 2013 June 13; 1514: 12–17. doi:10.1016/j.brainres.2013.04.011. Rationale and Design of the Kronos Early Estrogen Prevention Study (KEEPS) and the KEEPS Cognitive and Affective Sub