Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
02-4882–mc
MINERVA CHIR 2008;63:79-91
Maxillary sinus lift through heterologous bone grafts
and simultaneous acid-etched implants placement
Five year follow-up
D. STIEVANO 1, D. A. DI STEFANO 2, M. LUDOVICHETTI 3,
S. PAGNUTTI 4, F. GAZZOLA 5, C. BOATO 6, E. STELLINI 7
Aim. The aim of this study was to assess retro-
1Private practice (dentist), Vigonza, Italy
spectively at 5 years the clinical outcome of
bone regeneration in patients who underwent
maxillary sinus lift with different equine-
derived, enzyme-deantigenated equine bone
grafts, and simultaneous placement of acid-
faele Scientific University Institute
Ateneo Vita-Salute, Milan, Italy
3Private practice (dentist), Padua, Italy
4Biologist, Padua, Italy
etched surface implants.
Methods. Eighteen patients (10 males and 8
females, age between 55 and 61 years) were A
5Private practice (dentist), Treviso, Italy
6Private practice (dentist), Vicenza, Italy
7Department of Surgical and Medical Specialties
considered. They wer
University of Padua, Padua, Italy
e divided into 2 groups
according to the type of bone graft used: a com-
bination of an equine flexible heterologous
spongy bone layer (Osteoplant® Flex, Bioteck)
and equine heterologous cortical and spongy
the type of implants used allowed to achieve a
granules (Bio-Gen® Mix, Bioteck), group A, or
satisfying rate of success according to the cur-
a block of equine heterologous spongy bone
rent standards in implantology.
(Bio-Gen® Block, Bioteck), group B. Surface-
Key words:
Atrophy – Maxillary sinus –Dental
treated implants ("TRE" type, Biotec) were
placed simultaneously to sinus augmentations
and usual clinical and radiological tests were
performed at 6 months and every year up to 5
years after surgery.
The restoration of aesthetics and function
of the compromised denture through
Results. At 5 years, 45 out of 49 total implants
implant rehabilitation has become, in the lat-
placed (91.8%) were successful according to
the Albrektsson and Zarb criteria. The loss of
ter 10 years, a common practice also for the
the 4 failed implants was observed in 2 patients
less experienced dentist. This restorative
of group B during the first days following
approach leads inevitably to face clinical sit-
surgery.
uations of evident bone atrophy, which must
These results show that the het-
be overcome in order to make implant reha-
erologous bone grafts supported properly the
bilitation possible.1, 2 Bone loss at the level
bone regeneration inside the sinuses, and that
of the pavement of the maxillary sinus is quitecommon.3 Such bone atrophy can be ade-
Received on October 4, 2007.
quately managed with classical techniques of
Accepted for publication on March 14, 2008.
guided bone regeneration, like the onedescribed by Tatum,4 and Boyne and James.5
Address reprint requests to: D. Stievano, Private dentist, Via
As far as the bone graft that can be used, cur-
Kennedy 4, 35010 Vigonza, Italy.
E-mail:
[email protected]
rent literature defines autologous bone as the
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
"golden standard" for all bone regeneration
up to now, has been reported in clinical lit-
surgeries.6-10 Autologous bone, in fact, has: a)
erature. So, the primary aim of the present
osteoconductive effect (the mechanical sup-
work is to assess retrospectively, at 5 years
port to vessels and cells that have to invade
after surgery the success rate of 49 implants
the grafted site); b) osteoinductive effect (the
placed during 18 maxillary sinus augmenta-
capability of stimulating, through endoge-
tion procedures with such heterologous bone
nous growth factors, both angiogenesis and
grafts. Moreover, 2 different forms of such
morphogenesis); c) osteogenetic effect
equine-derived grafts, blocks or granules, are
(through the already differentiated, bone-
compared. Finally, this work is the first long-
producing osteoblasts it contains). Nonethe-
term clinical assessment of a novel type of
less, it is well known that the withdrawal of
acid-etched titanium implants.
autologous bone implies the need of open-ing a second surgery site, and this canincrease morbidity.11, 12 If the site of with-
Materials and methods
drawal is intraoral, the surgical and postsur-gical risk increase is lower, but the quantity
of bone is limited. On the contrary, if the siteis extraoral, the quantity of bone that can be
Eighteen patients (10 men and 8 women,
withdrawn is greater but the risk of morbid-
age between 55 and 61), featuring type 2
ity is much higher, postoperative pain can
mono- or bilateral sinusal bone atrophy
be significant, and proper surgery rooms are
according to the Favero-Brånemark classifi-
needed. These obstacles arising from the use
cation,24 were considered. All patients were
of autologous bone have led to the alterna-
in good general health; they were no smok-
tive choice of many non-autologous bone
ers or light smokers (less than 10 cigarettes a
grafts.6, 13-16 Among these, also mammal-
A
V day) and showed good oral hygiene condi-
derived heterologous bone is currently
exploited, since the non-organic mineral partof the bone of different mammals, including
Plan of grafts
Man, shows only slight differences in com-
All patients underwent maxillary sinus aug-
position and morphology 17 and, therefore,
mentation according to the Tatum and Misch 4
should show similar osteoclastic remodeling
procedure and were retrospectively divided
properties after being grafted. Thermally
into 2 groups according to the type of bone
(high-temperature) deantigenated bovine
substitute being used: either bone granules
bone has been widely used in maxillary sinus
and a flexible bone layer (group A, N=12, 6
augmentations,18, 19 providing successful clin-
men and 6 women), or bone blocks (group
ical outcomes but proving to be, nonethe-
B, N=6, 4 men and 2 women). The ridge
less, not or only very slowly remodeled by
MINER height in both groups was in the range 4.5 –
osteoclasts 20-22 probably because of a phys-
ical modification of bone apatite due to thethermal treatment itself. In order to overcome
Bone grafts
this limit, a low temperature (37 °C) deanti-
genation process, based on the use of diges-
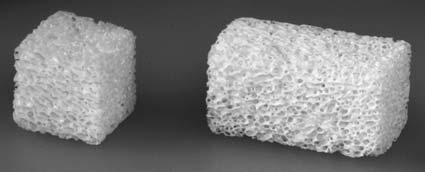
Bio-Gen MIX granules (BGM-05, Bioteck,
tive enzymes, has been devised to get phys-
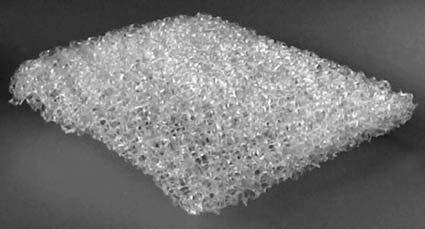
Italy) (Figure 1), Osteoplant Flex spongy flex-
iologically remodelable, totally deantigenic
ible bone layer (OTC-S1, Bioteck, Italy)
mammal-derived bone grafts. The enzymat-
(Figure 2) and Bio-Gen blocks (BGB-11,
ic process is currently applied to equine bone
10×10×10 mm or BGB-12, 10×10×20 mm,
Bioteck, Italy) (Figure 3), are all of equine
The clinical application of such bone grafts
origin. After cut and primary mechanical elim-
in maxillary sinus augmentation has already
ination of lipids, cortical or spongy bone sec-
been documented in a case report by De
tions undergo enzymatic deantigenation by
Biase
et al.,23 but no long-term follow-up has,
soaking them in thermostatically controlled
MINERVA CHIRURGICA

MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
Figure 2.—The heterologous (equine) enzyme-deanti-genated and demineralized (flexible) spongy layer
Figure 1.—The 50%-50% mixture of heterologous (equine)
(Osteoplant Flex, Bioteck), sized 25×25×3 mm.
enzyme-deantigenated cortical and spongy granules (Bio-Gen MIX, Bioteck).
enzymatic water-based solutions (37 °C, 1week). Such treatment allows achieving com-plete elimination of the organic componentaccording to the current ISO standard (ISO14493: 1991).
Bone sections used to get Bio-Gen blocks
are then deprived of bone collagen through a
Figure 3.—The heterologous (equine) enzyme-deanti-
wet high-pressure process (120 °C, 7 Bars).
genated spongy blocks (Bio-Gen Blocks, Bioteck), sized
Spongy blocks are finally cut according to the
10×10×10 or 10×10×20 mm, respectively.
desired size (10×10×10 mm or 10×10×20 mm). A
Granules are produced through mechanical
etched dental implants. Finally, "TRE"
grinding of cortical or spongy blocks. The
implants are sterilized through 25 kGy
granular mixture used in this study is a 50%-
50% commercial mixture of spongy and cor-tical granules, size from 0.5 to 1 mm. The flex-ible spongy layer, size 25×25×3 mm, instead,
is achieved by partially demineralising a deanti-
Presurgical preparation was performed
genated block, still containing bone collagen,
administering orally, as a systemic antibiotic
through an electrolytic acidic process.
875 mg amoxicillin and 125 mg potassium
Finally, all products are sterilized through
clavulanate (Augmentin, Glaxo Smith Kline,
25 kGy Beta-rays irradiation.
Italy) on the evening before surgery. One
MINER hour before surgery 2 mg diazepam were
administered orally (Valium 2, Roche, France)
"TRE" type implants (Biotec Srl, Italy)
as a sedative. The patient was then covered
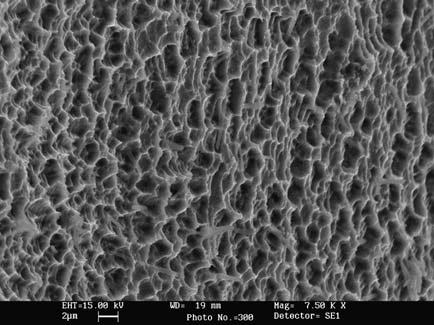
(Figure 4A) are acid-etched surface implants.
with sterile sheets and local anesthesia was
face is acid-etched twice in order to
performed with articaine (4%) and epineph-
achieve homogeneous micro-holes, whose
rine 1:100 000 (Citrocartin 100, Molteni, Italy).
average size is about 2 µm (Figure 4B). This
Surgery began with a slightly vestibular
size is very close to values that were shown
crestal incision of the keratinized mucosa,
to prompt the initial attachment of
about 1 cm long. Then some distal and mesial
osteoblasts.25, 26 Implants are then polished
incisions were performed and a whole thick-
through plasma treatment, in order to achieve
ness flap was detached.
a clean, uncontaminated surface. The final
The lateral wall of the maxillary bone was
degree of surface cleanness corresponds to
opened according to the "lateral window"
the one of other marketed high-level acid-
technique described by Tatum 4 and Boyne
MINERVA CHIRURGICA

MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTSTITOLO
Figure 4.—A) The Biotec "TRE" implant (the 3.75×13 mm model is showed). B) Its acid-etched surface (SEM, 7 500×).
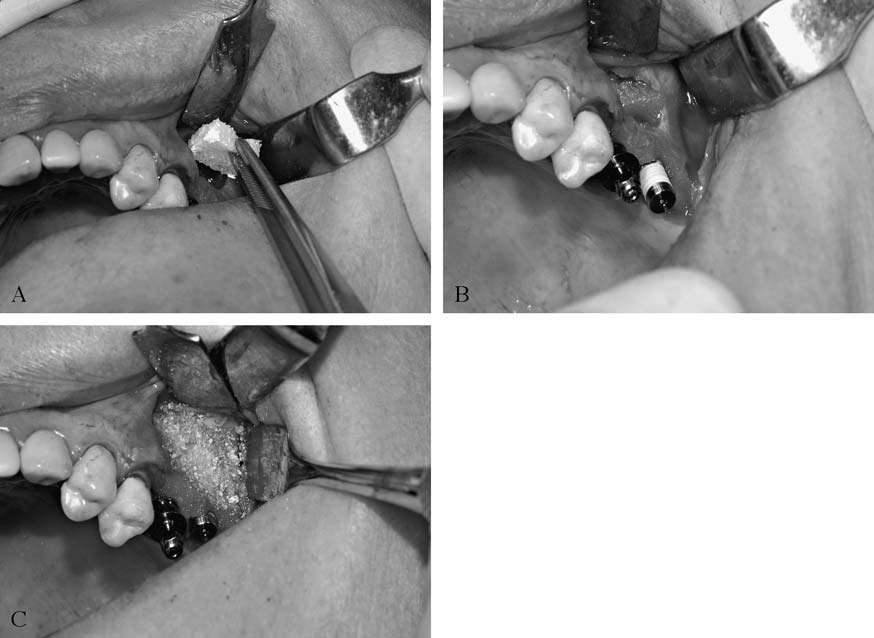
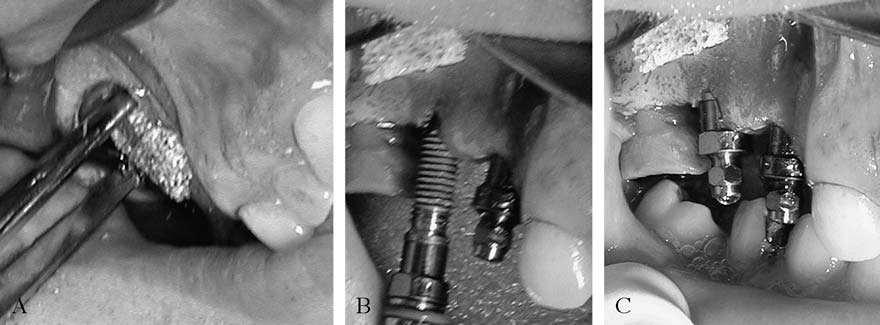
MINER Figure 5.—Sinus augmentation with granules and a flexible
spongy layer. A) The flexible layer is positioned to protectthe sinus membrane. B) Implants are placed. C) The cavi-ty is filled with granules.
and James.5 After opening an elliptical win-
to create a roof for the cavity in which the
dow sized approximately 8×12 mm, the sinus
bone graft would be placed.
membrane was detached using proper lifters
When the mixture of heterologous spongy
(SinusSet, Dentsply Friadent). The vestibu-
and cortical granules and the spongy flexible
lar window was then carefully moved
layer granules were used (Figure 5), they
towards the medial wall of the sinus in order
were hydrated separately with physiological
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
Figure 6.—Sinus augmentation with spongy block. A) The block is placed into the cavity and held still with the pliers.
B) and C) Implants are placed, after drilling the ridge and the block together.
solution for 3-4 min. The spongy layer was
days after surgery, twice a day (16 mg methyl-
then shaped with sterile scissors and was
prednisolone, Medrol, Pfizer, Usa). Patients
inserted through the bone window while
were also prescribed 20 mg piroxicam
holding it bent with pliers. In this way, after
(Brexin, Chiesi, Italy) for one day after
insertion in the cavity, it opened inside it and
sur MEDICA
gery, and they were advised to continue
lifted and protected the Schneider membrane.
treatment on the following days only if need-
The cavity was then partially filled with gran-
ed. Patients were also advised to use a spray
ules, and the ridge was drilled with the prop- A
V nasal decongestant (betamethasone 0.05g
er drills for implant placement. Implant(s)
and chlorohydrate tetrahydrozoline 0.1 g,
were placed and filling of the cavity with
Biorinil, Farmila-thea Farmaceutici, Italy) if
granules was completed.
needed, in order to avoid nose blowing and
In the alternative approach (Figure 6), the
the possible consequent disturbance to the
heterologous block was firstly hydrated for 3-
grafted site.
4 min by soaking it in physiological solution,
Sutures were removed after 10 days.
and then it was shaped with a blur to adapt
Prosthetic rehabilitation followed after 8-9
it to the grafting site. It was then inserted in
the cavity and, while holding it still with pli-ers, the ridge and the block were drilled
together with the proper drill for implant
MINER Patients were controlled once a month for
insertion. Then implant(s) were placed.
6 months and then every year up to 5 years,
If necessary, a continuous periosteal inci-
through clinical evaluation and panoramic
sion was performed to connect the vertical,
X-ray. Implant success or failure were
mesial and distal incisions in order to release
assessed through the Albrektsson and Zarb 27
totally the flap and to suture it with no ten-
criteria (the outcome is successful if the
sion. Suture was performed with vertical mat-
implant is stable and unless bone resorption
tress stitches, and single stitches (GoreTex,
exceeds 1.5 mm in the first year or 0.2 mm in
subsequent evaluations).
The same antibiotic treatment previously
described (Augmentin, Glaxo Smith Kline,Italy) was continued for 5 days after surgery,
twice a day. Immediately after surgery thepatient was given a tablet of an anti-inflam-
Outcome regarding group A and group B
matory drug that was prescribed also for 4
are summarized in Tables I and II, respec-
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
TABLE I.—Results - Group A (heterologous granules and spongy flexible layer).
3.75
3.75 MEDICA
TABLE II.—Results - Group B (bone blocks).
MINER Diameter of Length of Failure (F)
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
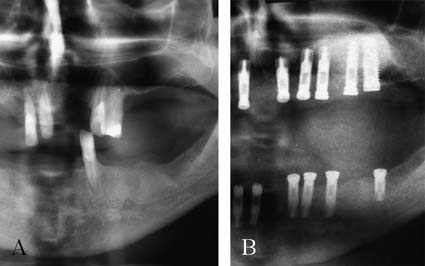
Figure 7.—Panoramic X ray: successful graft with gran-ules and flexible spongy layer. A) Before surgery. B) At 5years after surgery.
Figure 8.—Panoramic X-ray: successful graft with blocks.
A) Before surgery. B) At 5 years after surgery.
tively. Clinical outcome in groups A and B isas follows: group A (N=12, granules and flex-
Del Fabbro et al.28 (92.2%, 1 to 7 years follow-
ible layer), absolute complications 0%, rela-
up) and Wallace et al.29 (91.8%, 1 year mini-
tive complications 0%, no complications
mum follow-up), and represents a satisfying
100%; group B (N=6, blocks), absolute com-
clinical outcome.
plications 28.6% (4 implants over 14), relative
These results support the preliminary data
complications 0%, no complications 71.4%.
achieved by De Biase et al.23 about the use of
The absolute complications of group B
the same enzyme-deantigenated equine
patients appeared immediately after surgery:
spongy bone block to perform sinus aug-
on the first 2 days after surgery 2 patients A
V mentation. Their data, supported also by his-
complained about pain and exhibited sinusi-
tological examination, suggested that spongy
tis, and/or wound opening, with no response
block could be a good alternative to the use
to further administration of different antibi-
of autologous bone. According to our X-ray
otics. The grafted site was then reopened
results (Figures 7, 8), the radiographic appear-
and, in both cases, bone blocks were elimi-
ance of augmented sinuses either when the
nated. The 4 implants previously placed, 2 for
blocks or the granules and the flexible layer
each patient, were obviously lost.
were used, is quite similar to the one of the
Example X-rays of the different outcomes
surrounding endogenous bone. This radi-
observed, successful graft with granules and
ographic feature was visible already at one
flexible spongy layer and successful graft
year after grafting surgery.
with blocks, are shown in Figures 7 and 8,
This suggests that the heterologous grafts
underwent total or nearly total osteoclastic
At 5 years, according to the criteria of
remodeling, as showed in De Biase et al.23
Albrektsson and Zarb,27 failure of implants
and, as a consequence, that the low-temper-
was observed in 4 cases over 49, giving a
ature deantigenation method does not alter
percentage of success equal to 91.84%.
the remodeling properties of the mineral partof mammal bones. Anyway, more detailedhistological analyses are needed to assess
the actual remodeling rate of these bone sub-stitutes.
The survival rate of implants observed in
As far as the failures observed, we believe
this study is very close to the one observed
that they were caused by a lack of sufficient
in extensive reviews of literature about sinus
contact between the bone block surfaces and
augmentation procedures. In particular, it is
the vital bone of the patient. Such lack of
comparable with the values calculated by
contact with sufficient vital endogenous bone
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
could have hindered the correct spreading
blocks can lead to failure if there is no suffi-
of new blood vessels into the block itself,
cient contact surface between the block itself
making its osseointegration impossible and
and the vital bone of the patient. These
leading to failure. According to the personal
results, anyway, should be confirmed by clin-
experience of one of the authors (Boato),
ical split-mouth studies regarding a greater
the outcome when blocks are used to graft
number of patients.
the sinus is predictable only if the residual
Finally, the "TRE" implants used in this study
height of the ridge is not smaller than 5 mm,
proofed to give a success rate comparable to
and if at least 3 faces of the blocks are in
the one observed for other high-level implants
contact with vital, non-atrophic bone of the
in sinus augmentation procedure, confirming
patient. This would imply that bone blocks
that their acid-etched surface and the plasma
should be used only after a careful selection
polishing treatment of the surface itself can
of the patient, according to the residual bone
provide successful osseointegration.
thickness and the sinus anatomy (a CT should
We conclude that the use of Bio-Gen and
be preferred in these cases).
Osteoplant enzyme-deantigenated equine
Moreover, the results described in this
bone grafts in association with the simulta-
paper show that the implants that were used
neous placement of type "TRE" implants is
allowed achieving, at 5 years after surgery, a
clinically effective for the rehabilitation of
satisfying survival rate. The survival rate
the maxillary ridge when type 2 atrophy
observed, infact, is comprised in the range of
(according to Favero-Branemark 24 classifi-
successful survival rates that can be found
cation) is diagnosed.
in current clinical literature.30 This is in accor-dance with the current knowledge about
implant surfaces, which envisages a betterosseointegration for roughened-surface
1. Mericske-Stern RD, Taylor TD, Belser U. Management
of the edentulous patient. Clin Oral Implants Res
A2000;11(Suppl 1):108-25.
2. Hobkirk JA. Advances in prosthetic dentistry. Prim
Dent Care 2002;9:81-5.
V 3.Smiler DG, Johnson PW, Lozada JL, Misch C, Rosenlicht
JL, Tatum OH Jr et al. Sinus lift grafts and endosseousimplants. Treatment of the atrophic posterior maxilla.
The results of this study show that Bio-
Dent Clin North Am 1992;36:151-86.
Gen (granules and blocks) and Osteoplant
4. Tatum OH Jr. Maxillary and sinus implant reconstruc-
Flex heterologous bone grafts, deantigenat-
tions. Dent Clin North Am 1986;30:207-29.
5. Boyne PJ, James RA. Grafting of the maxillary sinus
ed through an enzymatic, 37 °C, system,
floor with autogenous marrow and bone. J Oral Surg
allowed achieving clinical success of implant
6. Barone A, Crespi R, Aldini NN, Fini M, Giardino R,
rehabilitation at five years after maxillary
Covani U. Maxillary sinus augmentation: histologic and
sinus augmentation, confirming the results
histomorphometric analysis. Int J Oral Maxillofac Impl2005;20:519-25.
previously achieved in the case report of De
7. Block MS, Kent JN. Sinus augmentation for dental
Biase et al.23 Moreover, according both to
implants: the use of autogenous bone. J Oral Maxillofac
clinical outcome and to X-ray examinations,
Surg 1997;55:1281-6.
8. Burchardt H. Biology of bone transplantation. Orthop
the results indicate that these bone substi-
Clin North Am 1987;18:187-96.
tutes underwent osteoclastic remodeling and
9. Buser D, Bragger U, Lang NP, Nyman S. Regeneration
total or nearly total substitution with endoge-
and enlargement of jaw bone using guided tissue regen-eration. Clin Oral Implants Res 1990;1:22-32.
nous bone over years. Anyway this behavior,
10. Friedlander G. Current concepts review: bone grafts: the
even if already observed by De Biase et al.,23
basic science rational for clinical application. J Bone
should be confirmed by further studies based
Joint Surg 1987;69:786-90.
11. Seiler JG 3rd, Johnson J. Iliac crest autogenous bone
on histological tests on a greater number of
grafting: donor site complications. J South Orthop
samples of regenerated bone.
Assoc 2000;9:91-7.
12. Kline RM Jr, Wolfe SA. Complications associated with
The results regarding the alternative use
the harvesting of cranial bone grafts. Plast Reconstr
of granules together with the flexible spongy
Surg 1995;95:5-13; discussion 14-20.
layer or bone blocks seem to indicate that
13. Aro HT, Aho AJ. Clinical use of bone allografts. Ann
Med 1993;25:403-12.
the first approach is preferred, since using
14. Hoffman HT, Harrison N, Sullivan MJ, Robbins KT,
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
Ridley M, Baker SR. Mandible reconstruction with vas-
stitute? J Long Term Eff Med Implants 1998;8:201-9.
cularized bone grafts. A histologic evaluation. Arch
23. De Biase A, Guerra F, Cipriano L, Lamazza L, Tucci E.
Otolaryngol Head Neck Surg 1991;117:917-25.
Subantral filling by deantigenated heterologous bone
15. Vanassche BJ, Stoelinga PJ, de Koomen HA, Blijdorp PA,
and immediate fixture placement. Minerva Stomatol
Schoenaers JH. Reconstruction of the severely resorbed
mandible with interposed bone grafts and hydroxyla-
24. Favero GA , Branemark PI. Il rialzo del pavimento del
patite. A 2-3 year follow-up. Int J Oral Maxillofac Surg
seno mascellare e l'osseointegrazione. Ed. Giornale di
Stomatologia e Ortognatodonzia, luglio 1994.
16. Wheeler SL. Sinus augmentation for dental implants: the
25. Lossdorfer S, Schwartz Z, Wang L, Lohmann CH, Turner
use of alloplastic materials. J Oral Maxillofac Surg
JD, Wieland M et al. Microrough implant surface
topographies increase osteogenesis by reducing osteo-
17. Pearce AI, Richards RG, Milz S, Schneider E, Pearce
clast formation and activity. J Biomed Mater Res A
SG. Animal models for implant biomaterial research
in bone: a review. Eur Cell Mater 2007;13:1-10.
26. Schwartz Z, Lohmann CH, Oefinger J, Bonewald LF,
18. Hallman M, Sennerby L, Zetterqvist L, Lundgren S. A 3-
Dean DD, Boyan BD. Implant surface characteristics
year prospective follow-up study of implant-support-
modulate differentiation behavior of cells in the
ed fixed prostheses in patients subjected to maxillary
osteoblastic lineage. Adv Dent Res 1999;13:38-48.
sinus floor augmentation with a 80:20 mixture of depro-
27. Albrektsson T, Zarb G, Worthington P, Eriksson AR.
teinized bovine bone and autogenous bone Clinical,
The long-term efficacy of currently used dental
radiographic and resonance frequency analysis. Int J
implants: a review and proposed criteria of success. Int
Oral Maxillofac Surg 2005;34:273-80.
J Oral Maxillofac Implants 1986;1:11-25.
19. Cornelini R, Cangini F, Martuscelli G, Wennstrom J.
28. Del Fabbro M, Testori T, Francetti L, Weinstein R.
Deproteinized bovine bone and biodegradable barri-
Systematic review of survival rates for implants placed
er membranes to support healing following immediate
in the grafted maxillary sinus. Int J Periodontics
placement of transmucosal implants: a short-term con-
Restorative Dent 2004;24:565-77.
trolled clinical trial. Int J Periodontics Restorative Dent
29. Wallace SS, Froum SJ. Effect of maxillary sinus aug-
mentation on the survival of endosseous dental
20. Skoglund A, Hising P, Young C. A clinical and histologic
implants. A systematic review. Ann Periodontol
examination in humans of the osseous response to
implanted natural bone mineral. Int J Oral Maxillofac
30. Hallman M, Mordenfeld A, Strandkvist T. A retrospec-
Implants 1997;12:194-9.
tive 5-year follow-up study of two different titanium
21. Sartori S, Silvestri M, Forni F, Icaro Cornaglia A, Tesei
implant surfaces used after interpositional bone graft-
P, Cattaneo V. Ten-year follow-up in a maxillary sinus
ing for reconstruction of the atrophic edentulous max-
augmentation using anorganic bovine bone (Bio-Oss).
illa. Clin Implant Dent Relat Res 2005;7:121-6.
A case report with histomorphometric evaluation. Clin
31. Albrektsson T, Wennerberg A. Oral implant surfaces:
Oral Implants Res 2003;14:369-72.
APart 2. Review focusing on clinical knowledge of dif-
Schlegel AK, Donath K. Bio-Oss-a resorbable bone sub-
ferent surfaces. Int J Prosthodont 2004;17:544-64.
Rialzo di seno mascellare attraverso innesti ossei eterologhi
e contemporaneo posizionamento di impianti a superficie mordenzata.
Follow-up a 5 anni
l recupero dell'estetica e della funzione della den-
ti gli interventi di rigenerazione ossea 6-10. L'osso auto-
tatura compromessa attraverso la riabilitazione
logo, infatti, possiede sia: a) effetto osteoconduttivo
implantare è divenuto, negli ultimi 10 anni, una pra-
(sostegno meccanico a vasi e cellule che devono inva-
tica comune anche per il dentista meno esperto.
dere il sito di innesto), b) effetto osteoinduttivo (la
L'approccio restaurativo conduce inevitabilmente a
capacità di stimolare, attraverso fattori di crescita endo-
confrontarsi con quadri clinici di evidente atrofia oseea,
geni, sia l'angiogenesi che la morfogenesi), e c) effet-
che devono essere superati per rendere possibile la ria-
to osteogenico (attraverso gli osteoblasti producenti tes-
bilitazione implantare 1, 2. La perdita di tessuto osseo
suto osseo già differenziati in esso contenuti). Tuttavia,
a livello del pavimento del seno mascellare è piutto-
è ben noto che il prelievo di osso autologo implica la
sto comune 3. Questa atrofia ossea può essere gestita
necessità di un secondo sito chirurgico, il che può
adeguatamente con tecniche classiche di rigenerazio-
portare ad un aumento della morbilità 11, 12. Se il sito
ne ossea guidata, come quella descritta da Tatum 4 e
di prelievo è intraorale, l'aumento del rischio intra e
Boyne e James 5. Per quanto riguarda l'innesto osseo
postoperatorio è ridotto, ma la quantità di tessuto
che può essere utilizzato, la letteratura corrente iden-
osseo che può essere prelevata è ridotta. Al contrario,
tifica l'osso autologo come il golden standard per tut-
se il sito di prelievo è extraorale, la quantità di tessu-
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
to osseo che può essere prelevata è maggiore, ma la
ta da Tatum e Misch4 e sono stati retrospettivamente
morbilità aumenta notevolmente, il dolore postope-
divisi in 2 gruppi in relazione al tipo di sostituto osseo
ratorio può essere significativo ed è necessaria una
utilizzato: granuli ossei e lamina ossea flessibile (grup-
sala operatoria opportunamente attrezzata. Questi limi-
po A, N=12, 6 uomini e 6 donne); oppure blocchi
ti nell'uso del tessuto osseo autologo hanno portato a
ossei (gruppo B, N=6, 4 uomini e 2 donne). L'altezza
scegliere, come alternativa, molti differenti innesti
della cresta residua era, per entrambi i gruppi, com-
ossei non autologhi 6, 13-16. Tra questi viene utilizzato
presa tra 4,5 e 5,5 mm.
attualmente anche il tessuto osseo di mammifero, inquanto la parte minerale anorganica del tessuto osseodelle diverse specie di mammifero, Uomo incluso,
Innesti ossei
mostra solo piccole differenze di composizione emorfologia 17 e di conseguenza dovrebbe esibire pro-
I granuli d'osso Bio-Gen MIX (BGM-05, Bioteck)
prietà simili di rimodellamento osteoclastico. Il tessu-
(Figura 1), la lamina ossea flessibile Osteoplant Flex
to osseo bovino, deantigenato per via termica (ad alta
(OTC-S1, Bioteck) (Figura 2), e i blocchi Bio-Gen
temperatura), è stato ampiamente utilizzato per gli
(BGB-11, 10x10x10 mm o BGB-12, 10x10x20mm,
interventi di rialzo di seno mascellare 18, 19, con risul-
Bioteck) (Figura 3), sono tutti di origine equina. Dopo
tati clinici soddisfacenti, pur essendo scarsamente o per
il taglio e una prima eliminazione meccanica dei lipi-
nulla rimodellato dagli osteoclasti 20-22, probabilmen-
di, le sezioni ossee, corticali o spongiose, sono sot-
te a causa di un'alterazione fisica dell'apatite ossea
toposte al trattamento enzimatico di deantigenazione
dovuta allo stesso trattamento termico applicato per
tramite immersione in soluzioni enzimatiche acquo-
ottenere la deantigenazione. Allo scopo di superare
se, in bagno termostatico (37 °C, 1 settimana). Questo
questo limite, è stato ideato un processo di deantige-
trattamento permette di ottenere l'eliminazione tota-
nazione a bassa temperatura (37 °C) basato sull'uso di
le della componente organica, secondo gli standard
enzimi digestivi, per ottenere innesti ossei derivati da
ISO attuali (ISO 14493:1991).
mammifero totalmente deantigenati e a rimodella-
Le sezioni ossee utilizzate per ottenere i blocchi
mento fisiologico. Questo processo è attualmene appli-
Bio-Gen sono quindi private del collagene osseo
cato, a livello produttivo, a tessuti ossei di origine
tramite un trattamento in fase umida ad alta pres-
sione (120 °C, 7 Bar). I blocchi spongiosi sono infi-
L'applicazione clinica di questi innesti nel rialzo del
ne sezionati per ottenere le misure desiderate
seno mascellare è già stato documentata in un caso A
(10x10x10 mm o 10x10x20 mm). I granuli sono pro-
clinico di De Biase et al.23
, ma ad oggi non è mai sta-
dotti per triturazione meccanica di blocchi spon-
to pubblicato un follow-up clinico a lungo termine. Lo
giosi o corticali. La formulazione granulare utilizza-
scopo principale di questo lavoro è quindi la valutazione
ta nel presente studio consiste di una miscela in
retrospettiva, a 5 anni dall'intervento, del successo di 49
parti uguali di granuli corticali e spongiosi, di dia-
impianti posizionati nel corso di 18 interventi di rialzo
metro medio compreso tra 0,5 e 1 mm. La lamina
di seno mascellare con tali innesti ossei eterologhi.
spongiosa flessibile, di dimensione 25x25x3 mm, è
Inoltre, in questo studio sono confrontate 2 differenti for-
ottenuta invece tramite demineralizzazione parzia-le di un blocco d'osso deantigenato, ancora conte-
me di tali innesti ossei di derivazione equina, blocchi
nente il collagene osseo, attraverso un processo
o granuli. Infine, questo lavoro rappresenta la prima
elettrolitico in ambiente acido.
valutazione clinica a lungo termine di un nuovo tipo di
Infine, tutti i prodotti sono sterilizzati attraverso
impianti in titanio a superficie mordenzata.
irraggiamento con raggi beta a 25 kGy.
Materiali e metodi
Gli impianti di tipo "TRE" (Biotec Srl) (Figura 4A)
sono impianti a superficie mordenzata. La superficie
Sono stati considerati 18 pazienti (10 uomini ed 8
è mordenzata 2 volte per ottenere delle micro-perfo-
donne di età compresa tra 55 e 61 anni), affetti da atro-
razioni omogenee il cui diametro medio è di circa 2
fia ossea sinusale mono- o bilaterale di grado 2 secon-
µm (Figura 4B). E' stato dimostrato che micro-fori di
do la classificazione di Favero-Brånemark 24. Tutti i
dimensione prossima a questo valore favoriscono l'a-
pazienti erano in buone condizioni generali di salu-
desione iniziale degli osteoblasti alla superficie
te, erano non fumatori o fumatori moderati (meno di
implantare 25, 26. Gli impianti sono quindi processa-
10 sigarette/die) e presentavano condizioni di buona
ti tramite un trattamento al plasma per ottenere una
superficie pulita e priva di contaminanti. Il gradofinale di pulizia della superficie corrisponde a quel-
Piano di trattamento
lo degli altri impianti mordenzati di fascia alta attual-mente in commercio. Infine, gli impianti "TRE" sono
Tutti i pazienti sono stati sottoposti a intervento di
sterilizzati attraverso irraggiamento a raggi gamma a
rialzo di seno mascellare secondo la procedura descrit-
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
Procedura clinica
dell'intervento è stata somministrata al paziente unacompressa di un antinfiammatorio che è stato pre-
La preparazione prechirurgica è stata eseguita som-
scritto anche per i 4 giorni successivi all'intervento, 2
ministrando oralmente, come antibiotico sistemico,
volte al giorno (metilprednisolone 16 mg, Medrol,
875 mg di amoxicillina e 125 mg di clavulanato di
Pfizer). Ai pazienti sono stati anche prescritti 20 mg
potassio (Augmentin, Glaxo Smith Kline) la sera pri-
di piroxicam per via orale (Brexin, Chiesi) per il gior-
ma dell'intervento. Un'ora prima dell'intervento sono
no successivo all'intervento, ed è stato consigliato di
stati somministrati per via orale 2 mg di diazepam
continuare il trattamento per i giorni successivi secon-
(Valium 2, Roche) come sedativo. Il paziente è stato
do necessità. E'stato inoltre consigliato ai pazienti,
quindi coperto con teli sterili, ed è stata eseguita l'a-
se necessario, di utilizzare un decongestionante nasa-
nestesia locale con articaina al 4% ed epinefrina 1:100
le spray (betametasone 0,05 g e tetraidrazolina clori-
000 (Citrocartin 100, Molteni).
drato 0,1 g, Biorinil, Farmila-thea Farmaceutici) per
L'intervento è iniziato con un'incisione in cresta,
evitare l'atto di soffiarsi il naso e le possibili conse-
leggermente vestibolare, della mucosa cheratinizza-
guenze negative nella sede dell'innesto.
ta, della lunghezza di circa 1 cm. Quindi sono state
Le suture sono state rimosse dopo 10 giorni. La
eseguite alcune incisioni di scarico, ed è stato distac-
riabilitazione protesica è stata portata a termine dopo
cato un lembo a tutto spessore.
La parete laterale del seno mascellare è stata aper-
ta secondo la tecnica della "finestra laterale" descrit-ta da Tatum 4, e Boyne e James 5. Dopo avere aper-
Criteri di valutazione clinica
to una finestra ellittica di dimensione approssimativa
I pazienti sono stati controllati una volta al mese per
di circa 8x12 mm, la membrana sinusale è stata sol-
6 mesi, e quindi ogni anno fino a 5 anni dall'inter-
levata utilizzando appositi scollatori (SinusSet,
vento, attraverso visita specialistica e radiografia pano-
Dentsply Friadent). La finestra vestibolare è stata
ramica. Il successo o il fallimento degli impianti sono
quindi gentilmente sollevata verso la parete mediale
stati valutati clinicamente secondo il criterio di
del seno al fine di creare un tetto per la cavità in cui
Albrektsson e Zarb 27 (stabilità meccanica dell'im-
è stato poi inserito l'innesto osseo.
pianto; l'entità del riassorbimento osseo perimplantare
Nei casi in cui sono stati utilizzati la miscela ete-
non deve essere maggiore di 1,5 mm il primo anno
rologa di granuli spongiosi e corticali e la lamina
e di 0,2 mm gli anni successivi).
spongiosa flessibile (Figura 5), essi sono stati idrata- A
ti separatamente in soluzione fisiologica per 3-4 min.
La lamina spongiosa è stata quindi sagomata con for-bici sterili ed è stata inserita attraverso la finestra
ossea tenendola parzialmente piegata con delle pin-zette. In questo modo, una volta all'interno della
I risultati relativi al gruppo A e al gruppo B sono
cavità la lamina si distendeva sollevando e proteg-
riepilogati rispettivamente in Tabelle I e II. Gli esiti del-
gendo la membrana di Schneider. Dopo avere riem-
la valutazione clinica a 5 anni per i gruppi A e B era-
pito parzialmente la cavità con la miscela granulare,
no i seguenti. Gruppo A (N=12, granuli e lamina fles-
la cresta è stata forata con le frese opportune per il
sibile): complicanze assolute 0%, complicanze relati-
posizionamento degli impianti, e gli impianti sono
ve 0%, nessuna complicanza 100%. Gruppo B (N=6,
stati inseriti. Infine, è stato completato il riempimen-
blocchi): complicanze assolute 28.6% (4 impianti per-
to della cavità con i granuli.
si su 14), complicanze relative 0%, nessuna compli-
Nell'approccio alternativo (Figura 6), il blocco ete-
rologo è stato prima idratato attraverso immersione in
Le complicanze assolute dei pazienti del gruppo B
soluzione fisiologica per 3-4 min, e quindi è stato
si sono manifestate immediatamente dopo l'inter-
sagomato con una fresa per adattarlo al sito di inne-
vento: nei primi 2 giorni 2 pazienti hanno lamentato
sto. E' stato posizionato all'interno della cavità e,
dolore e mostravano sinusite e/o riapertura del sito
tenendolo fermo con delle pinzette, è stato forato
innestato, e nessuna risposta a un'ulteriore sommi-
contemporaneamente alla cresta con l'apposita fresa
nistrazione di antibiotici differenti. Il sito innestato è
per il successivo inserimento degli impianti. Infine,
stato quindi riaperto e in entrambi i casi i blocchi
sono stati posizionati gli impianti.
ossei sono stati eliminati. I 4 impianti precedente-
Se necessario, è stata eseguita un'incisione perio-
mente posizionati, 2 per ciascun paziente, sono sta-
stale continua per collegare le incisioni verticali,
ti ovviamente perduti.
mesiali e distali, al fine di rilasciare completamente il
Radiografie di esempio dei risultati positivi osser-
lembo e poterlo suturare senza tensione. La sutura è
vati sono mostrate in Figura 7 (innesto con granuli e
stata eseguita con punti da materassaio verticali e
lamina flessibile) e Figura 8 (innesto con blocco).
punti staccati (GoreTex, WL Gore).
A 5 anni, secondo il criterio di Albrektsson e
Il trattamento antibiotico precedentemente descrit-
Zarb 27, sono stati dichiarati falliti 4 impianti su 49. La
to (Augmentin, Glaxo Smith Kline) è stato continua-
percentuale di successo corrispondente è pari al
to i 5 giorni successivi, 2 volte al giorno. Al termine
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
Il tasso di sopravvivenza degli impianti osservato
I risultati di questo studio mostrano che i sostituti
in questo studio è molto simile a quello osservato in
ossei eterologhi Bio-Gen (granuli e blocchi) e
revisioni estese della letteratura concernente la tecnica
Osteoplant Flex, deantigenati attraverso un processo
del rialzo di seno. In particolare esso è paragonabi-
enzimatico a bassa temperatura, hanno permesso di
le ai valori calcolati da Del Fabbro e Testori 28 (92,2%,
ottenere, a 5 anni, una riuscita riabilitazione implan-
follow-up da 1 a 7 anni) e da Wallace et al.29 (91.8%,
tare a seguito di interventi di rialzo di seno mascellare,
follow-up minimo di un anno), e rappresenta un
confermando i risultati precedentemente ottenuti nel
risultato clinico soddisfacente.
case clinico di De Biase et al.23. Inoltre, sia l'esito cli-
Questi risultati avvalorano i dati preliminari ottenuti
nico che gli esami radiografici indicano che tali sosti-
da De Biase et al.23 sull'utilizzo dello stesso blocco di
tuti ossei abbiano subito rimodellamento osteocla-
tessuto osseo equino spongioso deantigenato per via
stico e negli anni siano stati sostituiti completamen-
enzimatica per eseguire il rialzo di seno. Tali dati,
te, o quasi completamente, da tessuto osseo endo-
ricavati anche da opportuno esame istologico, sug-
geno. In ogni caso, questo comportamento, sebbene
gerivano che esso potesse essere una buona alter-
già osservato da De Biase et al.23, dovrebbe essere
nativa all'uso dell'osso autologo. Secondo i risultati
confermato da ulteriori studi basati sull'analisi isto-
radiografici da noi ottenuti (Figure 7, 8) l'aspetto
logica di un maggior numero di campioni di tessuto
radiografico dei seni rialzati sia con il blocco che con
osseo rigenerato.
i granuli e la lamina flessibile è molto simile a quel-
I risultati riguardanti l'uso alternativo o dei granu-
lo del tessuto osseo endogeno circostante. Tale aspet-
li e della lamina spongiosa flessibile, o dei blocchi
to radiografico era visibile già a un anno dall'inter-
ossei sembrano indicare che il primo approccio sia da
vento di innesto. Questo suggerisce che il tessuto
preferire, in quanto l'utilizzo dei blocchi può con-
osseo eterologo abbia subito rimodellamento osteo-
durre a fallimento se non vi è sufficiente superficie di
clastico totale o quasi-totale, come mostrato da De
contatto tra il tessuto osseo vitale del paziente e il
Biase et al.23 e, di conseguenza, che il metodo di
blocco stesso. Questi risultati, in ogni caso, dovreb-
deantigenazione a bassa temperatura non alteri le
bero essere confermati da studi su casi bilaterali, e su
proprietà di rimodellamento dei tessuti ossei di mam-
di un numero maggiore di pazienti.
Infine, si è osservato che gli impianti "TRE" utiliz-
Comunque, sono necessari studi istologici più det- A
V zati in questo studio hanno permesso di ottenere una
tagliati per valutare la reale cinetica di rimodella-
percentuale di successo, se inseriti contestualmente
mento di questi sostituti ossei.
all'intervento di rialzo di seno mascellare, paragona-
Per quanto riguarda i fallimenti osservati, ritenia-
bile a quella di altri impianti di fascia elevata, con-
mo che essi siano stati causati dall'assenza di suffi-
fermando che la superficie mordenzata ed il succes-
ciente contatto tra le superfici del blocco e l'osso
sivo trattamento al plasma della superficie stessa sono
vitale del paziente. Tale mancanza di contatto con
in grado di dare una efficace osteointegrazione.
sufficiente tessuto osseo endogeno vitale potrebbe
In conclusione, l'impiego dei sostituti ossei etero-
avere impedito la corretta propagazione dei nuovi
loghi deantigenati per via enzimatica Bio-gen ed
vasi sanguigni all'interno del blocco osseo, rendendo
Osteoplant, in associazione con l'inserimento simul-
l'osteointegrazione impossibile e portando al falli-
taneo di impianti tipo "TRE" è clinicamente efficace
mento. Per esperienza personale di uno degli Autori
per la riabilitazione della cresta mascellare quando è
(Boato), l'esito dell'impiego di un blocco per il rial-
diagnosticata un'atrofia ossea di tipo 2 secondo la
zo di seno mascellare è predicibile solo se l'altezza
classificazione di Favero-Branemark 31.
residua della cresta non è inferiore a 5 mm, e se alme-no tre facce del blocco sono in contatto con tessutoosseo vitale, non atrofico, del paziente. Questo impli-cherebbe che i blocchi d'osso dovrebbero essere uti-
lizzati solo in seguito a un'attenta selezione del pazien-
te, in funzione dello spessore osseo residuo e dell'a-
Obiettivo. Lo scopo di questo studio è valutare
natomia sinusale (in questi casi sarebbe preferibile
retrospettivamente dopo 5 anni l'esito clinico di inter-
eseguire una TAC preliminare).
venti di rialzo di seno mascellare attraverso l'innesto
Inoltre, i risultati descritti in questo articolo mostra-
di differenti sostituti ossei di origine equina, deanti-
no che gli impianti utilizzati hanno permesso di otte-
genati per via enzimatica e contestuale inserimento di
nere, a cinque anni dall'intervento, un tasso di soprav-
impianti a superficie mordenzata.
vivenza implantare soddisfacente. Esso, infatti, è com-
Metodi. Sono stati considerati 18 pazienti (10 uomi-
preso nell'intervallo di valori che può essere reperi-
ni e 8 donne, di età compresa tra i 55 e i 61 anni),
to nella letteratura clinica corrente 30. Questo è in
classificati in 2 gruppi in funzione del tipo di innesto
accordo con le conoscenze attuali sulle superfici
osseo utilizzato: una combinazione di una lamina ossea
implantari, che prevedono una migliore osteointe-
spongiosa flessibile eterologa equina (Osteoplant®
grazione per gli impianti a superficie trattata 31.
Flex, Bioteck) e granuli di osso corticale e spongioso
MINERVA CHIRURGICA
MAXILLARY SINUS LIFT THROUGH HETEROLOGOUS BONE GRAFTS
eterologo equino (Bio-Gen® Mix, Bioteck), gruppo
stata osservata in due pazienti del gruppo B, a pochi
A, o un blocco di osso spongioso eterologo equino
giorni dall'intervento.
(Bio-Gen® Blocco, Bioteck), gruppo B. Contestual-
Conclusioni. I risultati mostrano che i sostituti ossei
mente all'intervento di rialzo di seno, sono stati posi-
eterologhi utilizzati in questo studio hanno supportato
zionati, in tutti i pazienti, impianti a superficie mor-
correttamente la rigenerazione ossea nei seni mascel-
denzata (tipo "TRE" , Biotec). Gli usuali esami clinici e
lari, e che il tipo di impianti impiegati hanno per-
radiologici sono stati eseguiti a 6 mesi dall'intervento,
messo di ottenere una percentuale di successo sod-
e ogni anno fino a cinque anni dopo l'intervento.
disfacente secondo i parametri di riferimento attuali
Risultati. A 5 anni, 45 impianti su 49 (il 91,8%)
in implantologia.
erano stabili e funzionali secondo il criterio di
Parole chiave: Atrofia ossea - Seno mascellare -
Albrektsson e Zarb. La perdita dei 4 impianti falliti è
Materiali da innesto - Impianti a superficie.
MINERVA CHIRURGICA
Source: http://www.heliosmedical.ro/media/documente/080515_PA_MINCH_stie_EN_D.pdf.pdf
CHRONIC MEDICINE BENEFIT APPLICATION FORM – 2013 (To be used by Nedgroup Hospital, Traditional, Savings and Platinum members only) Please complete the application in black ink One application form must be completed per patient Please attach a copy of the Dr's prescription to the application form (original not required) Applications will not be processed unless the appropriate sections are completed and relevant documents are attached. The completed and signed application form may be faxed to 086 679 1579, emailed to or posted to Scriptpharm Risk Management, P.O. Box 653590, Benmore, 2010
Net feed intake: Potential selection tool to improve feed efficiency in beef cattle Gordon E. Carstens Department of Animal Science Texas A&M University Introduction: Recent economic analysis of standardized performance assessment (SPA) data from Texas, New Mexico and Oklahoma cow-calf operations (McGrann, 2002) revealed that grazing and feed costs per cow had a greater impact on determining net income per cow than weaning rates, calf weaning weights or pounds of calf weaned per cow exposed. Likewise, analysis of Iowa and Illinois SPA data found that total feed costs accounted for over 50% of the herd-to-herd variation in net income per cow. Results from these SPA databases illustrate that improvements in feed efficiency would significantly impact unit costs of production and improve profitability of cow-calf enterprises, thereby improving the competitiveness and long-term sustainability of the beef industry.