Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Sfed.org
Resolution™ Clip
Global Technique Spotlight
Naveen Arya, M.D.
Halton Healthcare Services, Oakville, Ontario, Canada
Marco Carniel, M.D.
Landesklinikum Wiener Neustadt, Wiener Neustadt, Austria
Nestor Chopita, M.D.,
Bárbara Agustina Amendolara, M.D.,
Francisco Tufare, M.D. and Nelson Condado, M.D.
Hospital San Martín de La Plata, Buenos Aires, Argentina
Robert S. Dean, M.D.
Vassar Brothers Medical Center
Poughkeepsie, NY, USA
Robert D. Fanelli, M.D., F.A.C.S.
Berkshire Medical Center and Surgical
Specialists of Western New England, P.C., USA
David A. Florez, M.D.
Elms Endoscopy Center/ Trident Gastroenterology,
Charlestown, South Carolina, USA
Francisco Igea, M.D.
Hospital Rio Carrion, Palencia, Spain
Houssam Kharrat, M.D.
Covenant Medical Center, Lubbock, TX, USA
Luis F. Lara, M.D.
The University of Texas
Southwestern Medical Center at Dallas, USA
Adolfo Parra-Blanco, M.D.
Canarias University Hospital, Santa Cruz de Tenerife, Spain





CLOSURE OF A PERFORATION AFTER
CLOSURE OF AN IATROGENIC PERFORATION AFTER
A SALINE-ASSISTED POLYPECTOMY
AN ENDOSCOPIC MUCOSAL RESECTION
Naveen Arya, M.D.
Marco Carniel, M.D.
Gastroenterology and Therapeutic Endoscopy Department, Halton Healthcare Services, Oakville, Ontario, Canada
Head of Endoscopy, Landesklinikum Wiener Neustadt, Wiener Neustadt, Austria
An 87-year-old male presented with a three month history of rectal bleeding. The
A 72-year-old female was referred to our centre for an endoscopic mucosal
patient had no weight loss, change in bowel habit or abdominal pain. His past
resection. The patient has a history of coronary heart disease, st.p. myocardial
medical history was relevant for coronary artery disease with coronary bypass,
infarction in 2000, arterial hypertension, hyperlipidaemia and osteoporosis.
hypertension and hyperlipidemia. He was on Coumadin™, Altace™, Lipitor™ and
In February 2005, the referring hospital performed a partial rectal polypectomy. In
Atenolol. Upon examination, the abdomen was found to be obese.
the last pre-colonoscopy examination, a recurrent flat polypoid formation wasdiscovered in the rectum.
The patient had a colonoscopy carried out by a general surgeon and was found to
have an 8cm rectal mass. The biopsy proved to be a tublovillous adenoma with high
An approximately 2.5cm flat adenoma could be seen in the rectum at 8cm. In the
grade dysplasia and the patient was referred for a polypectomy. The risks of the
centre of the lesion, scar tissue after the partial polypectomy in 2005 was readily
procedure such as perforation, bleeding or serious side effects were discussed with
distinguishable (Figure 1).
the patient and he consented to the procedure.
Fluid infiltration of the polyp revealed good lifting sign. Utilising a straight suction
The polyp was endoscopically removed with saline-assisted injection in a piecemeal
cap, the lesion was totally resected in four fragments using a piecemeal technique
fashion (Figure 1). The edges were coagulated with Argon plasma coagulation at
with a cautery snare.
40W (Figure 2). During the procedure it was noted that the middle of the
A 12mm perforation was revealed upon retrieval of the last fragment (Figure 2).
polypectomy base was open and the plane was obviously through the submucosa
By applying 7 Resolution™ Clips, the perforation edges could be properly aligned
(Figure 3). The base of the polyp was then clipped closed with 16 Resolution™ Clips
step-by-step and the perforation successfully closed (Figures 3, 4 and 5).
(Figures 4, 5 and 6).
After the procedure the patient was taken to recovery, given antibiotics IV and three
views of the abdomen were taken with no free air seen. The patient was stable andwanted to go home. He was put on PO antibiotics for seven days. The patient was
Flat tubular partially tubulovillous adenoma with low to moderate grade intraep-
seen within one week and had no symptoms or signs of perforation and was stable.
ithelial neoplasia, the muscularis mucosae overall intact – resection in toto.
The patient was kept under clinical observation for several days. There was no
Six months later, the patient had a flexible sigmoidoscopy and there was no
increase of inflammatory parameters upon serological examination and no clinical
evidence of residual polyp. A scar was found and biopsies taken from it revealed
signs of peritonitis. After two days, the patient was introduced to a dietary regimen
normal mucosa.
which was well tolerated. A surgical intervention was not necessary and after
This case demonstrates the utility of clips and gives endoscopists another modality
four days the patient was discharged.
to increase their therapeutic arsenal.
Coumadin™ is a trademark of Bristol-Myers Squibb. Altace™ is a trademark of King Pharmaceuticals. Lipitor™ is a trademark of Pfizer.
TREATMENT OF POST-EMR BLEEDING
PREVENTION OF POST-POLYPECTOMY
WITH ENDOSCOPIC CLIPS
HAEMORRHAGE USING THE RESOLUTION CLIP DEVICE
Nestor Chopita, M.D., Bárbara Agustina Amendolara, M.D.,
Robert S. Dean, M.D.
Francisco Tufare, M.D., Nelson Condado, M.D.
Vassar Brothers Medical Center, Poughkeepsie, NY
Gastroenterology Department, Hospital San Martín de La Plata, Buenos Aires, Argentina
A 62-year-old male with cirrhosis (Child B) and a history of variceal bleeding was
A 91-year-old man presented with a history of anaemia and haematochezia. The
admitted to our hospital for gastric polyposis resection.
patient was on chronic anticoagulation therapy with Coumadin™ due to porcine
mitral valve replacement. Other past medical history includes a two vessel
CABG, TIA, and seizure disorder. A colonoscopy was deemed necessary to
explore potential sources of hematochezia. Concern was given in particular to the
The endoscopy showed gastric polyposis and there was an abnormal area of
need for continuing anticoagulation therapy. The patient was counselled to
mucosa on the gastric incisura. Biopsy taken from the site revealed intra-mucosal
discontinue his Coumadin therapy five days prior to the scheduled colonoscopy.
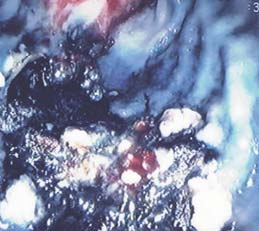
carcinoma and an endoscopic mucosal resection was performed (Figure 1).
Low-molecular-weight heparin was used to maintain anticoagulation until the
The patient had haemodynamic instability, haematemesis and haematocrit
evening prior to the procedure.
dropped at 22% 12 hours after the procedure. Another endoscopy showed active
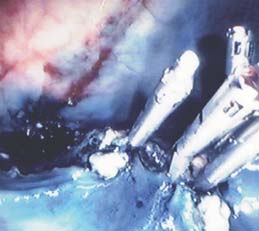
bleeding in the EMR site (Figure 2). The bleeding was successfully managed with
the use of two Resolution™ Clips (Figures 3 and 4).
A colonoscopy was performed, during which time a 2cm polyp, on a thick stalk,
was observed in the descending colon. This polyp was removed using a
Captivator™ II Single - use Snare and cautery techniques. Reinspection of the
During the follow up, the patient was in good condition and there were no
resection margin revealed pooling of fresh blood at the polyp stalk base (Figure 1).
complications (Figure 5). Histological results confirmed early gastric cancer (EGC).
Two Resolution™ Clips were places at the polyp stalk base with good
haemostasis (Figures 2 and 3).
Low-molecular-weight heparin was resumed the morning after the procedure.
There was no residual bleeding from the colon noted. Coumadin therapy
was resumed 14 days post procedure and the patient has not had any
Coumadin™ is a trademark of Bristol-Myers Squibb.
PREVENTION OF
MANAGEMENT OF A LARGE GASTRIC POLYP
Robert D. Fanelli, M.D., F.A.C.S.
David A. Florez, M.D.
Director of Surgical Endoscopy, Berkshire Medical Center and Surgical Specialists of Western New England, P.C.
Medical Director, Elms Endoscopy Center/Trident Gastroenterology, Charlestown, South Carolina
A 73-year-old man presented for outpatient consultation because of progressive
An 81-year-old woman was referred for evaluation of weight loss and persistent
dysphagia. During the consultation, it was discovered that he had not yet
nausea. Prior attempts at managing her symptoms with proton pump inhibitor
undergone screening colonoscopy. With his consent, he was scheduled for
therapy and promotility agents by her primary physician had failed. An EGD
sequential oesophagogastroduodenoscopy and colonoscopy in the outpatient
demonstrated a large gastric polyp at the pylorus (Figure 1), causing a functional
endoscopy unit.
gastric outlet obstruction. Radial Jaw™ 3 Standard Capacity Biopsy Forceps
showed the polyp to be a benign hyperplastic inflammatory polyp. She was
subsequently referred to me for endoscopic ultrasound evaluation (EUS) of the
polyp and possible gastric polypectomy for definitive therapy.
The upper endoscopy revealed a distal oesophageal reflux-related stricture.
Biopsies were taken using Radial Jaw™ 3 Large Capacity Forceps and then the
stricture was dilated using an 18-19-20mm CRE™ Fixed Wire Balloon Dilator
without incident. Screening colonoscopy revealed, what appeared to be, seven
The patient underwent EUS examination. The gastric polyp was scanned with a
adenomatous polyps distributed throughout the colon. One of the polyps was a
radial echoendoscope, revealing a large mucosal based lesion (Figure 2). There
long, slender, finger-like polyp in the proximal ascending colon (Figure 1). When
were no significant blood vessels within the polyp. Additionally, there were no
cautery snare polypectomy was performed, the substance of the polyp was
malignant features and no evidence of invasion to deeper layers of the gastric
stripped off of the underlying arterial structure that was central to its stalk (Figure
wall. No significant celiac or peri-gastric lymphadenopathy was appreciated.
2). The vessel was not bleeding or visibly pulsing, but was turgid and standing
A standard EGD scope was then passed and the polyp was removed in a piece-
erect. It was felt that this vessel would definitely start bleeding at some point
meal fashion with a Sensation™ Polypectomy Snare. The polyp fragments were
soon (Figure 3). A single Resolution™ Clip was placed across the vessel at the
then withdrawn through the mouth with a basket retrieval device.
base of the polyp, closing and reopening the clip until the perfect location was
The polypectomy ulcer was then re-inspected. There was mild, persistent oozing
identified to occlude the vessel. The Resolution Clip was then deployed. The
of blood at the site. Given the patient's advanced age and the fact that she
artery was immediately deflated and collapsed as the blood pressure within the
lived in a rural area with considerable drive time to the nearest medical facility,
structure was reduced to zero, virtually eliminating the risk of delayed
I elected to attempt primary closure of the site with Resolution™ Clips. The defect
polypectomy site haemorrhage. The shrivelled-up artery collapsed at the base of
edges were reapproximated with three Resolution Clips achieving adequate
the polyp, just above the Resolution Clip (Figure 4).
haemostasis. The patient tolerated the procedure well and there were no
peri-operative complications. Twice daily proton pump inhibitor therapy
was prescribed.
Pathologic inspection of the polyps removed during this screening colonoscopy
revealed three tubular adenomas and four tubulovillous adenomas. No
post-polypectomy haemorrhage occurred, and the patient's dysphagia was
Final pathologic diagnosis of the polyp revealed a benign inflammatory
completely abated after oesophageal dilation and the institution of proton pump
polyp without dysphagia. On follow up, the patient's nausea had resolved and
inhibitor therapy.
her weight had normalised.
CLOSURE OF AN IATROGENIC COLON
BLEEDING DIVERTICULUM CLOSURE
PERFORATION WITH ENDOSCOPIC CLIPS
Francisco Igea, M.D.
Houssam Kharrat, M.D.
Gastroenterology Department, Hospital Rio Carrion, Palencia, Spain
Gastroenterologist, Covenant Medical Center, Lubbock, TX
An 82-year-old woman with abdominal pain and change in bowel habits was
An 83-year-old man presented with shortness of breath, generalised weakness
remitted to our endoscopy unit for a total colonoscopy. The procedure was done
and had been passing bright red blood from his rectum for 48 hours.
under continuous propofol sedation. A difficult and angulated sigma was noticed
Past medical history was significant for Chronic Obstructive Pulmonary Disease
and multiple attempts in different positions were done. During one advancing
(COPD), Chronic Heart Failure (CHF) and Hypertension (HTN). Patient was treated
manoeuvre, an iatrogenic perforation was noticed.
with blood pressure medication and ASA 81mg daily. Vital signs and physical
exam appeared normal at the time of admission. Labs showed: WBC 7.3, Hgb 9.2,
hematocrit 26.8, platelets 211 and an INR of 0.97. The patient had a negative
A big hole showing mesenteric fat and vessels was seen (Figure 1). Immediate
bleeding scan and was prepped for a colonoscopy the following day.
suction in order to minimise pneumoperitoneum and close the hole was applied
(Figure 2). The first Resolution™ Clip was placed closing the lips of the hole
(Figure 3). Then another two Resolution Clips were placed until complete suture of
Patient prep was suboptimal. No active bleeding was seen, diverticulosis was
the perforation was achieved (Figures 4 and 5).
observed up to the cecum, and bright red blood was found in the right colon. An EGD
was performed, to rule out an upper-GI source of the bleeding, which was
unremarkable. The patient was transfused and a repeat colonoscopy was done
The patient was admitted to our hospitalisation unit and nil
the following day.
per os and I.V. fluids and antibiotics (cefuroxime and
A bleeding diverticulum was noted in the sigmoid colon (Figures 1 and 2). An
metronidazol) were given, two hours later, an abdominal
injection of epinephrine 1:10000 did not control the bleed. A Resolution™ Clip
CT scan with contrast enema was done showing no
was used to approximate the diverticulum edge. A total of six Resolution Clips
leakage (Figures 6, 7 and 8). Pneumoperitoneum and
(Figures 3 and 4) were deployed successfully to close the edge of the diverticulum.
retropneumoperitoneum was clearly demonstrated. Only
slight pain was present during the first 48 hours.
The patient reintroduced oral intake 72 hours later and
Good haemostasis was established at the end of the procedure. The patient
was discharged seven days after without further
did not require any additional transfusion and he was discharged shortly after.
A three month follow up did not show any evidence of bleeding.
One month later the patient was doing fine without
BLEEDING FROM A COLON TUMOUR AFTER
TREATMENT OF MUCOSAL TEARS IN THE
BIOPSY WITH FORCEPS
OESOPHAGUS WITH ENDOSCOPIC CLIPS
Luis F. Lara, M.D.
Adolfo Parra-Blanco, M.D.
Assistant Professor of Internal Medicine
Department of Gastroenterology, Canarias University Hospital, Santa Cruz de Tenerife, Spain
Division of Digestive and Liver Diseases, The University of Texas, Southwestern Medical Center at Dallas
A 42-year-old white male diagnosed with cystic fibrosis, who had a bilateral lung
A 73-year-old male underwent an upper endoscopy for the study of long-standing
transplant in 1997 with a single previous episode of rejection and diabetes
reflux symptoms. The examination was done under conscious sedation with poor
mellitus, was referred to evaluate episodic mild haematochezia and new onset
tolerance, in spite of the administration of 100 µg of fentanyl and 7 mg of
constipation requiring intermittent laxative use. The patient had a previous
Midazolam, and nausea occured repeatedly during the procedure.
spontaneous diverticular perforation for which he had a diverting colostomy that
During the initial passage of the endoscope in the oesophagus, a long segment
had been repaired three years earlier.
of Barrett's oesophagus was detected, with no other gross abnormalities. Onwithdrawal, two tears were found in the lower end of the columnar epithelium,
proximally to the cardia: a shallow 1cm tear (located at 6 o'clock – Figure 1) and a
The colonic anastomosis appeared normal. A circumferential, friable mass
deep 3cm tear (located at 3 o'clock – Figure 1).
occluding the lumen to about 12mm and measuring 4cm in length was seen in the distal transverse colon. A standard biopsy forceps was used to biopsy
the mass (Figure 1). Bleeding continued from one of the biopsy sites (estimated
The affected area was flushed with water in order to have a clear view of the lesion.
to be 8mm in size), which did not stop after five minutes of irrigation and
The bottom of the tear was inspected in detail and no signs of perforation were
observation (Figure 2). A Resolution™ Clip was used to approximate the sides
evident. There was some oozing from the tear and a decision was made to suture
of the biopsy site, achieving haemostasis, which was confirmed before
the mucosal defect in order to prevent further complications such as delayed
scope withdrawal (Figure 3). Follow-up confirmed there was no further bleeding
bleeding or perforation.
Five Resolution™ Clips were applied and attached consecutively in a distal toproximal order (Figure 2). The reason for this is that the clips initially applied may
hamper the precise application of further clips, and it is easier to check the mucosal
defect remaining to be sutured if the direction is from distal to proximal. This aspectis important, because although clipping is considered to be almost devoid of anyrisks, there is a possibility that a clip incorrectly placed at the bottom of a mucosaldefect instead of grasping normal mucosa at the edge of the lesion can result in a perforation.
The tear was successfully sutured with five Resolution Clips, which were placedeasily (Figure 3). The extent of the Barrett's oesophagus was C5M8 according to thePrague Classification. No biopsies were taken to confirm the diagnosis. The patientremained asymptomatic and was discharged after observation.
The patient was on high dose PPI. Four months later in a second endoscopy, no
trace of the tear was found, but random biopsies revealed high-grade dysplasia in
the Barrett's epithelium. A third endoscopy was performed in order to try to locate
any dysplastic areas, and two small erosions were found in a Barrett's tongue
(Figure 4). Biopsy taken from both areas revealed high-grade dysplasia and an
endoscopic mucosectomy is planned.
Mucosal tears in the oesophagus may occur during diagnostic or therapeutic
endoscopy, but they are very infrequent and underlying conditions such as
eosinophilic oesophagitis should be ruled out. Resolution Clips are a valuable tool
for the management of intraprocedural complications (bleeding, and perforations).
These cases reflect the opinion of and are the responsibility of their respective authors.
European Distribution Centre –
India – Mumbai
South East Asia – Thailand
The N etherlands
T: +57 1 629 5045
F: +57 1 612 4761
T: +91 22 4030 9165
F: +91 22 4040 9199
T: +66 2 6380 100
F: +66 2 6380 400
T: +31 45 54 67 700
F: +31 45 54 67 800
South East Europe
European Headquarters –
T: +420 296 331 901
F: +420 296 331 935
T: +39 010 60 60 1
F: +39 010 60 60 200
T: +30 210 9542 300
F: +30 210 9542 310
Spain – Barcelona
T: +82 2 3476 2121
F: +82 2 3476 1776
T: +34 93 444 72 00
F: +34 93 405 90 45
Spain – Madrid
F: +5411 4896 8517
T: +52 55 5687 63 90
F: +52 55 5687 62 28
T: +34 901 11 12 15
F: +34 91 319 50 03
Middle East/Gulf/North Africa
T: +61 2 8063 8100
F: +61 2 9330 1404
T: +358 20 762 8882
F: +358 20 762 8883
T: +961 1 805 410
F: +961 1 805 445
T: +46 42 25 69 00
F: +46 42 25 69 69
F: +43 1 60 810 60
T: +31 30 602 55 44
F: +31 30 602 55 05
T: +41 32 626 57 00
F: +41 32 626 57 01
T: +886 2 2747 7278
F: +886 2 2747 7270
Turkey – Istanbul
T: +55 11 5502 8500
F: +55 11 5103 2212
T: +30 210 9542 300
F: +30 210 9542 310
T: +48 22 435 14 14
F: +48 22 435 14 10
T: +90 216 464 36 66
F: +90 216 464 36 67
Hong Kong
T: +1 888 359 9691
F: +1 888 575 7396
T: +852 2960 7100
F: +852 2563 5276
T: +351 1 381 25 40
F: +351 21 381 25 58
South Africa
T: +36 1 456 30 40
F: +36 1 456 30 41
T: +27 11 840 8600
F: +27 11 463 6077
T: +59 82 900 6212
F: +59 82 900 6212
China – Beijing
India – Bangalore
South East Asia – Malaysia
T: +86 10 8525 1588
F: +86 10 8525 1566
T: +91 80 2212 4928/9 F: +91 80 2207 5153
T: +60 3 2283 3813
F: +60 3 2284 3813
T: +58 212 959 6275
F: +58 212 959 5328
China – Guangzhou
India – Chennai
South East Asia – Philippines
T: +86 20 8767 9791
F: +86 20 8767 9789
T: +91 44 2220 1879
F: +91 44 2220 0716
T: +63 2 687 6994
F: +63 2 687 3047
China – Shanghai
India – Delhi
South East Asia – Singapore
T: +86 21 6141 5959
F: +86 21 6141 5900
T: +91 11 4243 2222
F: +91 11 2610 0808
RCS Nanterre B420 668 420 2008 Boston Scientific Corporation
All cited trademarks are the property of their respective owners. CAUTION: The law restricts these devices to sale by or on the order of a physician. Indications, contraindications, warnings and instructions for use
can be found in the product labelling supplied with each device. Information for the use only in countries with applicable health authority product registrations.
or its affiliates. All rights reserved.
PSST 5136 Printed in the UK by Gosling.
Source: http://www.sfed.org/files/documents_sfed/partenaires/bostonscientific/pdf/casclinique_resolution.pdf
helping families & friends find better ways Psychiatric medications finding the appropriate medication and • possible side effects and what should The experience of mental illness can have dosage, and in talking through concerns be done if they occur; a profound impact upon people's work, about side effects. • how long will it be necessary to take the family and social lives, as well as on
"Medicinal crops" in Ethiopia - Current status and future potentials- Japan Association for International Collaboration of Agriculture and Forestry In response to the Development Initiative which was proposed by the then Prime Minister Koizumi on the occasion of the WTO ministerial conference in Hong Kong in December 2005, the Ministry of Agriculture, Forestry and Fisheries has announced "the Initiative by Ministry of