Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Ortho0506battaglia.indd
Ossifi c Tendonitis of the Achilles with
Tendon Fracture: A Case Report and
Literature Review
TODD C. BATTAGLIA, MD; JAMES T. CHANDLER, MD
Ossifi c tendonitis has been de-
scribed in numerous anatomic sites, occasionally involving the
Achilles tendon. Although the fi rst report-ed cases of Achilles tendon ossifi cation appeared in the 1930s,1,2 fracture of an os-sifi ed Achilles tendon is a rare event, hav-ing been reported in the English literature �15 times.3-5 This article reports a patient with massive ossifi cation of his Achilles tendon, presumably related to a trauma from 25 years prior to presentation, who remained asymptomatic until a second
minor trauma resulted in fracture through
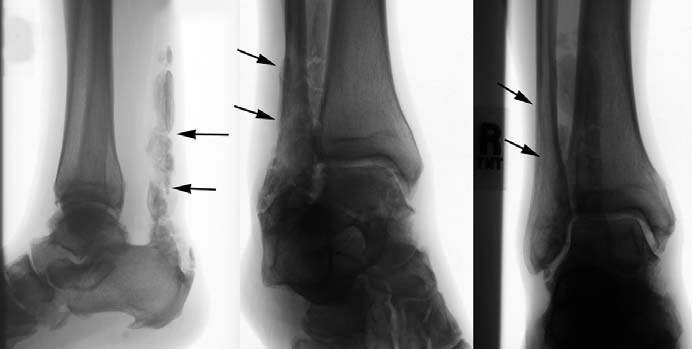
Figure 1: Lateral (A), mortise (B), and AP (C) radiographs of the ankle demonstrate diffuse ossifi cation of
the ossifi ed tendon. Pain relief and full the Achilles tendon with evidence of multiple fractures (arrows).
function were restored with tendon resec-tion and reconstruction with fl exor hallicis
signifi cant conditions were hypertension and
area (Figure 1). Blood analysis, including re-
longus tendon. To our knowledge, this is
hyperlipidemia, for which he took benazepril
nal function tests and calcium level, was un-
the fi rst reported use of fl exor hallicis lon-
hydrochloride and fenofi brate. He did not use
gus transfer for the treatment of extensive
tobacco products.
Over the next 3 months, nonoperative treat-
Achilles tendon ossifi cation with fracture.
On physical examination, there was fusi-
ment was attempted with full-time use of a
form swelling and fi rmness of the right Achil-
fi xed ankle walker and anti-infl ammatories.
CASE REPORT
les tendon extending from the tendon insertion
The patient reported pain relief while wearing
A 55-year-old man presented with a one-
to near the musculotendinous junction. No the brace, but suffered an immediate return of
week history of right heel pain after strain-
gross defects or areas of discontinuity were
ing his Achilles tendon while pruning a tree.
palpable. The left Achilles tendon was normal
Dr Battaglia is from the Department of Or-
Since the injury, he described increasing pain
in appearance and palpation. He was able to
thopedic Surgery, University of Virginia Health
and progressive diffi culty with ambulation. His
perform a single-leg toe rise on the left side,
Sciences Center, Charlottesville and Dr Chandler
medical history included a previous rupture of
but not on the right side, although Thompson's
is from the Roanoke Orthopedic Center, Roanoke, Va.
the right Achilles tendon from 25 years prior
calf squeeze test was normal bilaterally. Ra-
Reprint requests: Todd C. Battaglia, MD,
to presentation that had been treated non-op-
diographs demonstrated extensive ossifi cation
Dept of Orthopedic Surgery, University of Vir-
eratively and, per the patient, had healed un-
of the right Achilles tendon, with evidence of
ginia Health System, Box 800159, Charlottesville,
eventfully with no residual sequelae. Other multiple fracture lines through the pathologic
MAY 2006 Volume 29 • Number 5


to a short-leg walking cast. His ankle did not
reach neutral dorsifl exion at this point, and he
was immobilized in approximately 5� of equi-nus. Two weeks later, he was re-cast at neutral.
Nine weeks postoperatively, the cast was dis-
continued and he was placed in a fi xed ankle
walker with an adjustable heel lift that he wore
at all times except for daily ankle range of mo-
tion (ROM) exercises. At 14 weeks postopera-
tively, he reported no pain and reached 7� of ankle dorsifl exion. The boot was discontinued
and he was advanced to full weight bearing
with activity restrictions.
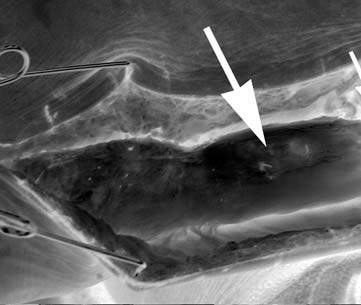
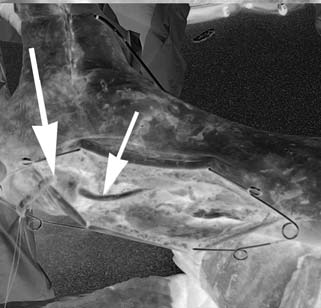
Figure 2: Intraoperative photographs of the extensively ossifi ed Achilles (large arrow) with more normal
tendon tissue seen adjacently (small arrow) (A) and transfer of the fl exor hallicis longus tendon (small
At 6-month follow-up, the patient was pain-
arrow) through a drill hole in the calcaneus (large arrow) after Achilles resection (B).
free but still unable to perform a single-leg heel
rise. Formal physical therapy was prescribed,
and by one year postoperatively, ankle ROM
was equivalent on the right and left, and the pa-
tient was able to perform a painless single-leg
heel rise. At 18 months postoperatively, the pa-
tient reports no pain or functional limitation.
DISCUSSION
Extra-articular calcifi cations can be found
around many joints in the body, most
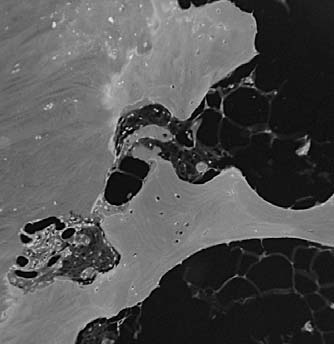
Figure 3: Gross (A) and microscopic pathology
commonly the shoulder, elbow, wrist, hip,
photographs (B) of a specimen showing osseous composition of the tendon.
and knee.3,7 Calcifi c tendonitis has been described in nearly every tendon site,
including the quadriceps muscles, wrist fl exors, spinal accessory muscles, pecto-
symptoms when the brace was weaned. Ulti-
ralis, trapezius, biceps, gluteus, piriformis,
mately, he was offered the option of tendon
popliteus, and peroneals. Calcifi c tendon-
debridement and reconstruction using fl exor
itis, however, must be distinguished from
hallicis longus tendon. This was performed 6
true ossifi c tendonitis. Calcifi cation refers
months after initial presentation. Intraopera-
to the deposition of amorphous calcium
tively, a large portion of the tendon was found
phosphate or carbonate, and occurs more
to be completely ossifi ed (Figure 2), with evi-
frequently in males between aged 25 to 60
dence of a partially healed fracture in its mid-
years.8 Nearly all calcifi c tendon deposits
substance. The abnormal section was resected
become absorbed or disappear over time.8
and reconstruction was performed by transfer-
Ossifi cation, however, refers to the forma-
ring the fl exor hallicis longus tendon to the cal-
tion of hydroxyapatite crystals in a his-
caneus as previously described by Wapner et
tologic pattern consistent with (and with
al6 (Figure 3). Pathologic examination of the
the biologic behavior of) mature lamel-
specimen confi rmed extensive ossifi cation of
lar bone.9 Like calcifi c tendonitis, ossifi c
the tendon (Figure 4). A postoperative radio-
tendonitis is also more prevalent in men,
graph is shown in Figure 5.
but has no known age predilection.10 The
Postoperatively, the patient was cast in Achilles tendon is often calcifi ed but rare-
equinus and maintained on strict non-weight-
ly ossifi ed,3 and only occasional reports
Figure 4: Postoperative radiograph demonstrat-
ing complete removal of the ossifi c portion of the
bearing precautions. His wound healed un-
of ossifi c Achilles tendonitis appear in the
Achilles tendon.
eventfully, and at 5 weeks he was transitioned
ORTHOPEDICS www.ORTHOSuperSite.com
OSSIFIC TENDONITIS OF THE ACHILLES TENDON BATTAGLIA AND CHANDLER
Most cases of Achilles ossifi cation are as-
surgical intervention. One surgical op-
2. Watson-Jones R. Ossifi cation of the Achilles
tendon. Brit Med J. 1932; 2:943.
sociated with a medical history of surgical
tion includes direct repair and fi xation
3. Fink RJ, Corn RC. Fracture of an ossifi ed
intervention or trauma.7,11 Other causes of the ossifi ed fragments, but the extent
Achilles tendon. Clin Orthop. 1982; 169:148-
of tendon ossifi cation may include neo-
of tendon involvement led us to recom-
plasm, chronic infection (such as syphilis,
mend excision of the diseased segments 4. Friedman L. Achilles tendon ossifi cation and
abscess, or osteomyelitis), renal disease, with tendon reconstruction. Numerous
fracture. S Afr Med J. 1991; 79:170.
Reiter's syndrome, and crystal arthropa-
soft-tissue options, including fascia lata, 5. Parton MJ, Walter DF, Ritchie DA, Luke LC.
Case report: fracture of an ossifi ed Achilles
thies.7,11-13 Two distinct patterns of os-
plantaris, fl exor digitorum longus, and
tendon - MR appearances. Clin Radiol. 1998;
sifi cation may be seen. The fi rst involves
peroneus brevis, have been described for
one or more large segments of mature Achilles reconstruction.3,11-13 Here, how-
6. Wapner KL, Pavlock GS, Hecht PJ, Naselli F,
bone with well-organized trabeculae and ever, we used the fl exor hallicis longus
Walther R. Repair of chronic Achilles tendon rupture with fl exor hallicus longus transfer.
distinct cortex, as often is seen after trau-
transfer as described by Wapner et al6 for
Foot Ankle. 1993; 14:443-449.
ma or in Wilson's disease, renal failure, the treatment of chronic Achilles rupture. 7. Raynor KJ, McDonald RJ, Edelman RD, Par-ochronosis, and spondyloarthropathies. To our knowledge, this is the fi rst reported
kinson DE. Ossifi cation of the Achilles ten-
The second pattern consists of multiple instance of fl exor hallicis longus transfer
don. J Am Podiatr Med Assoc. 1986; 76:688-690.
tiny foci or linear deposits within the ten-
to treat fracture of an ossifi ed Achilles
8. Rowe CR. Calcifi c tendinitis. Instr Course
don substance and is more common in tendon. The fl exor hallicis longus tendon
Lect. 1985; 34:196-198.
pseudogout and hemochromatosis.3,5,7 It is stronger than the fl exor digitorum lon-
9. Mady F, Vajda A. Bilateral ossifi cation in the
is hypothesized that ectopic endochondral
gus or peroneus brevis, and its excursion,
Achilles tendon: a case report. Foot Ankle Int. 2000; 21:1015-1018.
ossifi cation results from fi broblast migra-
strength, and contractile axis most closely
tion into areas of damage with subsequent
approximate the gastrocnemius-soleus 10. Lotke PA. Ossifi cation of the Achilles ten-
don: report of seven cases. J Bone Joint Surg
bone deposition in response to tissue hy-
complex.16 Despite potential complica-
Am. 1970; 52:157-60.
poxia.14 On magnetic resonance imaging,
tions, including loss of great toe interpha-
11. Weseley MS, Barenfeld PA, Eisenstein AL.
the signal characteristics of involved ten-
langeal fl exion and medial plantar nerve
Fracture of an ossifi c mass in the Achilles tendon. Bull Hosp Joint Dis. 1976; 37:159-
don are compatible with lamellar bone.5
injury during harvest, most studies report
Ossifi c Achilles tendonitis usually presents
excellent outcomes after fl exor hallicis
12. Haddad FS, Ting P, Goddard NJ. Successful
as a fi rm mass, but is often nontender and
longus transfer for other Achilles ten-
non-operative management of an Achilles
nonpainful until tendon rupture or fracture
donopathies. In this case, our patient ul-
fracture. J R Soc Med. 1999; 92:85-86.
occurs.10 Although some authors13 have
timately regained painless ROM and full 13. Kernohan J, Hall AJ. Treatment of a fractured
ossifi ed Achilles tendon. J R Coll Surg Edinb.
recommended surgical treatment for all function. We believe that, after failure of
1984; 29:263.
Achilles fractures, multiple reports exist nonoperative management, the fl exor hal-
Yu JS, Witte D, Resnick D, Pogue W.
describing successful nonoperative treat-
licis longus transfer is also an effective
Ossifi cation of the Achilles tendon: imaging
ment.4,11,12,15 Nonoperative management treatment in cases of fracture of an ossi-
abnormalities in 12 patients. Skeletal Radiol. 1994; 23:127-131.
probably is most appropriate if the tendon
fi ed Achilles tendon.
Banerjee A. Ruptured calcifi ed tendo
ends are not widely separated.4
Achilles: successful non-operative treatment.
Despite well-approximated tendon ends, REFERENCES
Injury. 1992; 23:496-497.
a three-month period of immobilization 1. Ghormley JW. Ossifi cation of the tendo 16. Kann JN, Myerson MS. Surgical manage-for this patient failed to produce clini-
Achilles. J Bone Joint Surg. 1938; 20:153-
ment of chronic ruptures of the Achilles ten-
don. Foot Ankle Clin. 1997; 2:535-545.
cal relief. Accordingly, we proceeded to
MAY 2006 Volume 29 • Number 5
Source: http://www.syracusesportsmedicine.com/pdf/ossific-tendonitis-of-the-achilles.pdf
The Hormone War is heating up The other day, I had my radio on. It was airin I was doing something else at the time, but there was one segment that caught my attention. "Deny, dismiss, delay. It's the same general strategy used by the tobacco industry and others to obfuscate issues and keep the public confused. And it's worked." I said to myself that's exactly what's been going on with the bio-identical vs fake hormone
SK is happy to present the Annual Report for the year 2010. The report endeavors to communicate to the readers the tasks accomplished by the organization over the defined period, the challenges met and Aalso the emerging issues it had to deal with. Needless to say it would not have been possible to achieve many of the goals without the assistance provided by different sections of people. Planning, Monitoring and Evaluation unit of ASK prepared the report by collecting and compiling information from different programmes. All the staff including the Executive Director and members went through the draft and commented upon it. ASK