Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Pone.0113936 1.15


Randomized Placebo-Controlled Phase IITrial of Autologous Mesenchymal StemCells in Multiple Sclerosis
Sara Llufriu1., Marı´a Sepu´lveda1., Yolanda Blanco1, Pedro Marı´n2,Beatriz Moreno1, Joan Berenguer3, In˜igo Gabilondo1, Eloy Martı´nez-Heras1,Nuria Sola-Valls1, Joan-Albert Arnaiz4, Enrique J. Andreu5, Begon˜a Ferna´ndez1,Santi Bullich1, Bernardo Sa´nchez-Dalmau1,6, Francesc Graus1, Pablo Villoslada1,Albert Saiz1*
Citation: Llufriu S, Sepu´lveda M, Blanco Y, Marı´n
1. Center of Neuroimmunology, Service of Neurology, Hospital Clinic and Institut d9Investigacions
P, Moreno B, et al. (2014) Randomized Placebo-
Biome diques August Pi i Sunyer (IDIBAPS), University of Barcelona, Barcelona, Spain, 2. Hemotherapy
Controlled Phase II Trial of Autologous
Service, CDB, Hospital Clı´nic, Barcelona, Spain, 3. Service of Neurorradiology, Hospital Clinic and Institut
Mesenchymal Stem Cells in Multiple
d9Investigacio´ Biome diques August Pi i Sunyer (IDIBAPS), University of Barcelona, Barcelona, Spain, 4.
Sclerosis. PLoS ONE 9(12): e113936. doi:10.1371/
Department of Clinical Pharmacology, Hospital Clinic, Barcelona, Spain, 5. Cell Therapy Area, Clinica
Universitaria de Navarra, Pamplona, Spain, 6. Service of Ophtalmology, Hospital Clinic, Barcelona, Spain
Editor: Tim Friede, University Medical Center
Go¨ttingen, Germany
. These authors contributed equally to this work.
Received: June 23, 2014
Accepted: October 29, 2014
Published: December 1, 2014
Copyright: ß 2014 Llufriu et al. This is an open-access article distributed under the terms of the, which
Objective: Uncontrolled studies of mesenchymal stem cells (MSCs) in multiple
permits unrestricted use, distribution, and repro-
sclerosis suggested some beneficial effect. In this randomized, double-blind,
duction in any medium, provided the original authorand source are credited.
placebo-controlled, crossover phase II study we investigated their safety and
Data Availability: The authors confirm that all data
efficacy in relapsing-remitting multiple sclerosis patients. Efficacy was evaluated in
underlying the findings are fully available without
terms of cumulative number of gadolinium-enhancing lesions (GEL) on magnetic
restriction. All relevant data are within the paperand its Supporting Information files.
resonance imaging (MRI) at 6 months and at the end of the study.
Funding: This work was supported by Ministerio
Methods: Patients unresponsive to conventional therapy, defined by at least 1
de Sanidad y Polı´tica Social [grant number TRA-066], Spain. The funder had no role in study
relapse and/or GEL on MRI scan in past 12 months, disease duration 2 to 10 years
design, data collection and analysis, decision to
and Expanded Disability Status Scale (EDSS) 3.0–6.5 were randomized to receive
publish, or preparation of the manuscript.
IV 1–26106 bone-marrow-derived-MSCs/Kg or placebo. After 6 months, the
Competing Interests: SL, MS, YB, PM, BM, JB,IG, EMH, NSV, JAA, JA, BF, SB, BSD and FG
treatment was reversed and patients were followed-up for another 6 months.
have nothing to declare. PV has received
Secondary endpoints were clinical outcomes (relapses and disability by EDSS and
consultancy fees from Novartis, Roche, Neurotek,Heidelberg Engineering, Digna Biotech, Bionure
MS Functional Composite), and several brain MRI and optical coherence
and TFS and research grants from Novartis, Rocheand Digna Biotech, and is founder and holds
tomography measures. Immunological tests were explored to assess the
stocks in Bionure. AS has received compensation
for consulting services and speaking from Bayer-Schering, Merck-Serono, Biogen-Idec, Sanofi-
Results: At baseline 9 patients were randomized to receive MSCs (n55) or
Aventis, Teva Pharmaceutical Industries Ltd and
placebo (n54). One patient on placebo withdrew after having 3 relapses in the first
Novartis. Dr. Pablo Villoslada, co-author of thepaper, is a PLOS ONE Editorial Board member.
5 months. We did not identify any serious adverse events. At 6 months, patients
This does not alter the authors' adherence toPLOS ONE Editorial policies and criteria.
treated with MSCs had a trend to lower mean cumulative number of GEL (3.1, 95%
PLOS ONE DOI:10.1371/journal.pone.0113936

Mesenchymal Stem Cells in MS
CI51.1–8.8 vs 12.3, 95% CI54.4–34.5, p50.064), and at the end of study to
reduced mean GEL (22.8¡5.9 vs 3¡5.4, p50.075). No significant treatment
differences were detected in the secondary endpoints. We observed a non-
significant decrease of the frequency of Th1 (CD4+ IFN-c+) cells in blood of MSCs
treated patients.
Conclusion: Bone-marrow-MSCs are safe and may reduce inflammatory MRI
parameters supporting their immunomodulatory properties.
ClinicalTrials.gov
Mesenchymal stem cells (MSCs) also called mesenchymal stromal cells, are bonemarrow-derived stem cells that can be relatively easily isolated from differenttissues, expanded ex vivo and induced to differentiate into mesodermal derivates.
Although MSCs therapies were originally based on the possibility to restoredamaged tissues, MSCs have emerged as a potential therapy for multiple sclerosis(MS) based on other properties than tissue replacement, such as their ability toinhibit pathogenic T and B cell responses and on the release of neuroprotectiveand pro-oligodendrogenic molecules favoring tissue protection and repair Preclinical studies on animal models of MS support both neuroprotection andimprovement of the clinical course after infusion of MSCs Five clinicalstudies on MS patients have shown the safety of the procedure at short-term andpreliminary efficacy results All studies, however, had an open-label design,and differed in the source, dose and way of MSCs administration, andcharacteristics of the series
On the basis of the consensus of the ‘‘International Mesenchymal Stem Cells
Transplantation Study Group'' (IMSCTSG) on the utilization of MSCs for thetreatment of MS we conducted a randomized, double-blind, crossover,placebo-controlled phase II trial with autologous MSCs transplantation in 9patients with relapsing-remitting MS (RRMS) using a similar protocol (EUDRA-CT: 2009-016442-74).
Patients and Methods
The protocol for this trial and supporting CONSORT checklist are available assupporting information; see Checklist S1, Protocol S1 and Protocol S2.
This randomized, double-blind, crossover placebo trial was performed in HospitalClinic of Barcelona, Spain, between November 2010 and June 2012. Patients wererandomized to receive intravenous injection (IV) of fresh bone-marrow-derived
PLOS ONE DOI:10.1371/journal.pone.0113936

Mesenchymal Stem Cells in MS
MSCs or equivalent volume of suspension media at baseline. At 6 months sincethe first infusion, treatment was reversed (i.e., patients who received initialsuspension media received cryopreserved MSCs and vice versa). Patientsunderwent bone marrow aspiration (80 to 100 ml) from the posterior-superioriliac spine under short general anaesthesia. Treatment sequence (active-control/control-active) was randomized following a computer-generated assignment list(M.A.S. v. 2.1, GSK). All patients and study personal, except for the haematologist(PM) and the nurse involved in the preparation of the dose and administration ofthe infusion, were blind to the treatment assignment at all timepoints, and untilthe last enrolled patient completed the 360-day visit, and all outcome data hadbeen processed.
Eligible participants were those with relapsing-remitting MS not responding to atleast a year of approved therapy, defined by at least 1 clinically documentedrelapse and/or at least 1 gadolinium-enhancing lesion (GEL) on MRI within thelast 12 months, aged 18 to 50 years, disease duration of 2 to 10 years andExpanded Disability Status Scale (EDSS) score between 3.0 to 6.5. Patientswere excluded if they had any active or chronic infection, treatment with anyimmunosuppressive therapy within the previous 3 months or interferon-beta,glatiramer acetate or corticosteroids within 30 days prior to randomization. Allpatients gave written informed consent before study entry and approval wasobtained from the Ethics Committee of Hospital Clinic of Barcelona. The trial wasregistered at ClinicalTrials.gov (NCT01228266) and the official protocol (inSpanish, EUDRA-CT: 2009-016442-74) is accurately described in the methods.
Study procedures and endpoints
MSCs were generated under good manufacturing practice conditions withstandard operating procedures. Briefly, the mononuclear cell fraction was isolatedby Ficoll density gradient centrifugation (Ficoll-Paque, GE Healthcare Bio-Sciences, AB). A number between 20–60 millions of mononuclear cells wereseeded per flask (175 cm2) with growth medium, which contained aMEMwithout ribonucleosides (Gibco), 5% platelet lisate, 2 un/ml Heparin, 1% Pen/Strep (Gibco) and 1 ng/ml human fibroblast growth factor (bFGF or FGF-2)(Sigma). The flasks were maintained in culture at 37˚C/5% CO2. The growthmedium was changed every 3–4 days. About 10–15 days later, colonies wereformed. Then the cells were splitted with TrypLE Select (Life Technologies) andseeded at 3000–5000 cells/cm2. The cells were grown to 70–80% confluence andsplitted again. When cellular doses were reached, the cells were resuspended at 10million cells/ml in Ringer Lactate buffer containing 1% Human Albumin.
Previously, the cells were analyzed by flow cytometry to confirm expression ofCD90, CD73 y CD44 and absence of CD34 and CD45 surface markers. The cellswere administrated in the first 24 hours postproduction (baseline) or cryopre-
PLOS ONE DOI:10.1371/journal.pone.0113936

Mesenchymal Stem Cells in MS
served for reversed administration at 6 months. A dose of 1–26106 MSCs/Kgbody weight or suspension media were slowly infused over 2–4 min through aperipheral venous cannula at baseline. At 6 months, treatment was reversedcompared to baseline and all patients received premedication with 2 mgdexchlorpheniramine, 1 g paracetamol, and 100 mg methylprednisolone toprevent infusion reactions.
Clinical assessmentsClinical assessments were performed at screening, and at randomization(baseline), and study visits, including safety assessments, were scheduled at 1, 3, 6,7, 9 and 12 months after randomization. Relapses were defined by one of theparticipant neurologists as the development of new neurologic symptoms andconfirmed signs at least 30 days after onset of last relapse. In case ofcorticosteroids treatment the MRI was delayed 1 month. The EDSS and theMultiple Sclerosis Scale Functional Composite (MSFC) z- score wereevaluated every 3 months.
MRI protocol and image analysisStandardized MRI images were obtained at the screening visit, at baseline andevery 3 months with a 3T Siemens Trio MRI scanner (Erlangen, Germany), usinga 32-channel head coil. Two blinded MRI raters (SL and JB) identified enhancinglesions on axial T1-weighted sequence after gadolinium injection (GEL) and newlesions or enlarging lesions on serially registered long repetition time images (T2/FLAIR sequences). The volumetric measures included normalized T2 lesionvolume, normalized gray matter volume, normalized white matter (WM) volumeand percentage of brain volume change. Additional non-conventional quantitativeMRI outcomes were used to evaluate the possible neuroprotective and repaireffects of MSCs such as magnetization transfer ratio of GEL and of normal-appearing WM (NAWM), diffusion tensor imaging of NAWM and N-acetylaspartate levels (for more details on the MRI methods see Appendix S1).
Optical coherence tomography (OCT)Spectral Domain retinal OCT (Spectralis, Heidelberg Engineering) was performedfor each eye based on previously reported protocols by a blinded trainedneurologist (IG) at baseline, after 6 and 12 months. Peripapilar Retinal NerveFiber Layer (RNFL) thickness and macular volume (MV) were obtained, and thevalues of each eye were used for the analysis.
Immunological evaluationPeripheral blood mononuclear cells (PBMCs) were isolated by densitycentrifugation (Ficoll-Paque Plus, GE Healthcare Life Sciences) from wholevenous blood of patients at baseline and every 3 months. 106 freshly isolatedPBMCs were plated overnight in sterile culture medium. The next day, PBMCswere activated with 2 ml/ml of cell culture, of leucocyte activation cocktail (BDPharmingen). After washing with phosphate-buffered saline, cells were fixed,permeabilized and stained to asses the frequency of Th1 (CD4+IFN-c+), Th17
PLOS ONE DOI:10.1371/journal.pone.0113936

Mesenchymal Stem Cells in MS
(CD4+IL17+), natural Treg (CD4+CD25+Foxp3+), induced Treg(CD4+CD3+IL10+) and Breg cells (CD19+IL10+) (see list of antibodies used inTable S1). Cells were analysed with a Beckman Coulter Gallios cytometer andFlow Jo software by a blinded researcher (BM) (Appendix S1).
EndpointsThe coprimary endpoints were safety of IV MSCs in RRMS patients and efficacyin terms of cumulative number of gadolinium-enhancing lesions (GEL) betweengroups of treatment during the first 6 months and the reduction in the meannumber of GEL (MSCs vs placebo period) at the end of the study. Secondaryendpoints included clinical outcomes (number of relapses, change in the EDSSand MSFC z- score), MRI-based measures (listed in the MRI protocol) and OCTmeasures between groups of treatment during the first 6 months and at the end ofthe study. Exploratory analysis included the immunological evaluation.
Statistical analysis
The trial was planned to randomize 16 patients as suggested by the IMSCTSG. Nopower calculation was attempted. However, the enrollment accrual of 0.7 patientsper month dropped 1 year after initiation, coincidental with the approval offingolimod as second line therapy in Spain, and only one more patient wasrandomized from November 2011 to June 2012 and it was decided to end therecruitment. Analysis was performed based on the intention to treat with lastobservation carried forward (LOCF) to impute missing values. The primaryendpoint of cumulative number of GEL at 6 months (sum of the number of GELon T1-weigthed MRI brain scans at months 3 and 6) was estimated by means of anegative binomial regression model with adjustment for baseline number ofGEL. A sensitivity analysis was also done without LOCF imputation for missingdata introducing as offset variable the natural log of the number of scansperformed in the first 6 months. Additionally, the effect of MSCs vs placebo onGEL at 6 months was also analyzed by Mann-Whitney U test as change in thenumber of GEL with respect to baseline. The primary endpoint of change in thenumber of GEL in the complete period of the study was analyzed by the non-parametric Wilconxon's rank test for paired samples (MSCs period vs placeboperiod). To identify a possible carryover effect of the MSCs therapy, we alsocompared the cumulative number of GEL during the first 6 months (sum of thenumber of GEL at months 3 and 6) and during the second 6 months (sum of thenumber of GEL at months 9 and 12). For those variables expressed as a change at6 months the analysis was calculated with respect to baseline. Treatmentcomparison for the secondary endpoints at 6 months and for the complete periodwas analyzed as reported in the primary MRI outcome. MSFC disability outcomewas analyzed by Z-score conversion as indicated. The statistical analysis ofimmunologic studies was performed using SPSS 17.0. Mixed effects modelsincluding carryover effect and subject as random variable was fitted to thefrequency of immune system cells in the blood flow versus the treatment (placebo
PLOS ONE DOI:10.1371/journal.pone.0113936

Mesenchymal Stem Cells in MS
or treatment with MSCs). A subdivision has been done regarding treatmentperiod (first period, from month 0 to month 6 or second period, from month 6 tomonth 12).
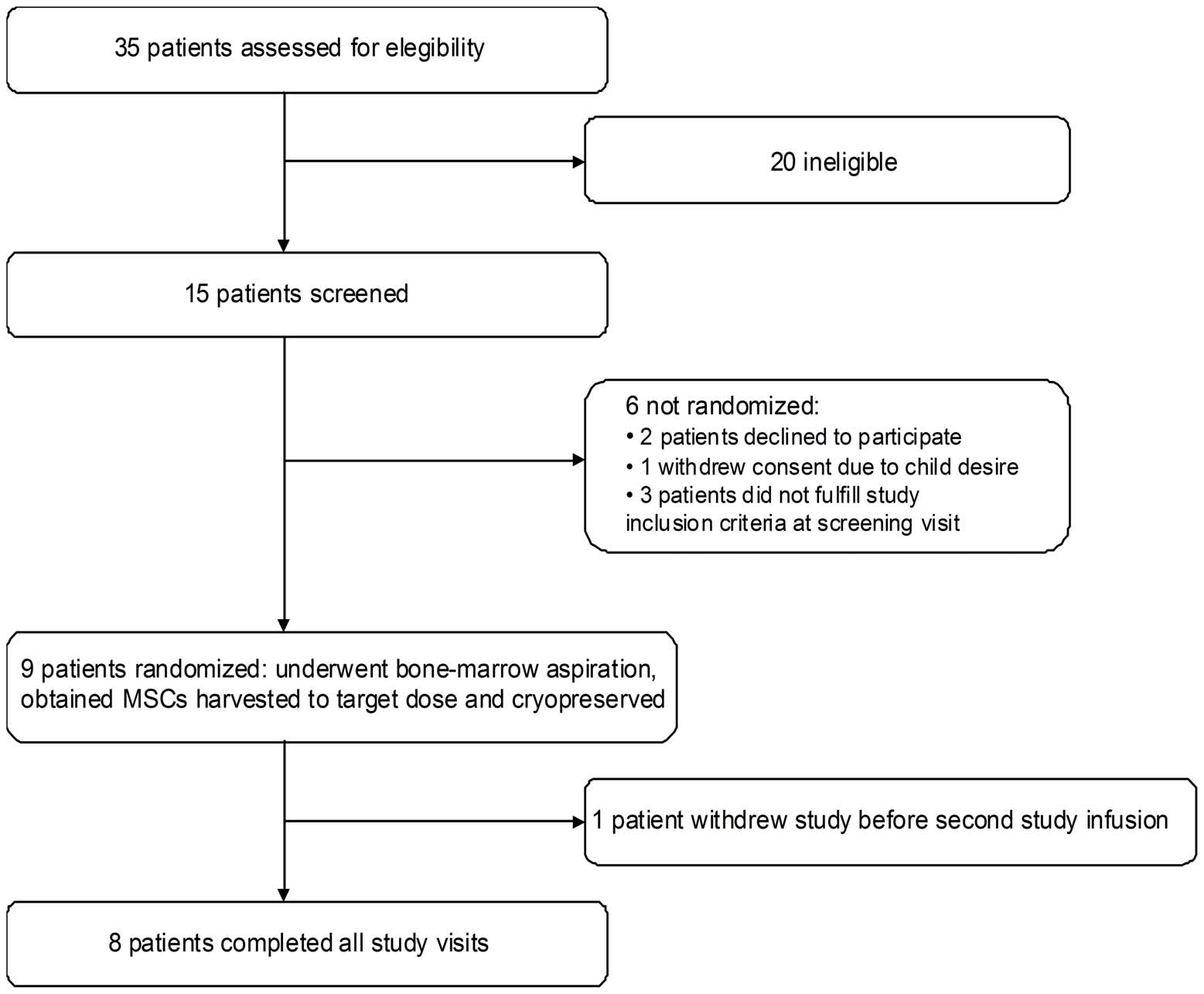
A total of 15 patients were assessed for eligibility, 10 were eligible and 9 patientswere enrolled in the study shows the study profile). shows thebaseline participants' characteristics.
Patient 9 failed to grow adequate number of MSCs. The patient had a relapse in
the interval of MSCs culture that was treated with IV methylprednisolone and a newbone marrow aspiration was successfully performed 6 weeks later. The mean cultureduration was 27 days (15–42). The mean administered dose was 1.876106 per Kgbodyweight (1.036106–2.166106). At baseline 4 patients received placebo and 5MSCs. There were not significant differences between both groups in demographicsor mean of GEL at baseline (4.75¡7.6 vs 4.6¡9.7, p51.0). Patient 1, randomizedto placebo in the first period, withdrew the consent after having 3 relapses in thefirst 5 months ). The patient completed all the safety evaluations.
Safety of MSCs therapy
Patient 4 had a facial flushing during infusion of placebo and was the only recordedadverse event (AE) related to infusion. The only severe AE reported was a femurfracture secondary to an accident and therefore it was considered as not related withthe therapy. During the placebo phase there were three upper respiratory infections,two gastroenteritis, and one dental abscess, and during the therapy phase one upperrespiratory infection, one influenza virus infection and one gastroenteritis, all ofthem graded as mild. Patient 7 had a herpes labialis 7 days after the first infusion and1 month after the second infusion. Results of blood testing were unremarkablealong the trial. We did not identify any delayed AE after completion of the 12months protocol (median follow-up 13 months; range, 1–19 months).
Efficacy of MSCs therapy
shows the individual clinical evolution. At 6 months, there was a trend to
lower mean of cumulative number of GEL in patients treated with MSCs (3.1,95% confidence interval [CI] 1.1–8.8 vs 12.3, 95% CI 4.4 to 34.5, p50.064). Thistrend was also confirmed after analyzing the mean change in the number of GEL(p50.06) (Additionally, the sensitivity analysis without the LOCFstrategy also showed a trend to lower accumulate number of GEL at 6 months inthe MSCs group (1.53, 95% CI 0.53–4.42 vs 6.15, 95% CI 2.19–17.28, p50.065).
At the end of the study the patients during the period of MSCs therapy had atrend to significant reduction in the mean number of GEL in comparison with theperiod of placebo (22.78¡5.89 vs 3¡5.36, p50.075) The analysis ofthe cumulative number of GEL between the first and the second period of
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
Figure 1. Study profile.
treatment showed a significant trend to lower mean number of GEL in the secondperiod suggesting a potential carryover effect of MSCs administration(13.33¡20.5 vs 9.78¡20.02, p50.066). No significant treatment differences weredetected in any of the secondary endpoints and Table S2; Table S3 showsthe number of GEL for each patient along the trial). Regarding clinical endpoints,4 patients had relapses (n57) during the placebo period. One of them withdrewthe study and did not receive MSCs (see before). Three patients had relapses(n54) during the MSCs period ((p50.11 at 6 months, and p50.6between both periods). The EDSS score increased 1.0 point in the patient whowithdrew the study, 0.5 points in one patient who had 1 relapse and decreased 0.5points in 2 patients who did not have relapses along the study. The rest remainedwithout changes. No significant differences in the EDSS or MSFC z-score changewas observed at 6 months and at the end of the study ().
Effects of MSCs therapy in T and B cell population frequency in blood
To assess the in vivo effects of MSCs therapy in the immune system of thepatients, we quantified the frequency of Th1 (CD4+IFN-c+), Th17 (CD4+IL17+),natural Treg CD4+CD25+Foxp3+), induced Treg (CD4+CD3+IL10+) and Breg cells
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
Table 1. Patients characteristics at baseline.
Number of patients
Gender ratio, Female/Male
Age (years); mean (SD)
Disease duration (years); mean (SD)
Relapses in previous 2 years; mean (SD)
Relapses in the last year; mean (SD)
Annualized relapse rate; mean (SD)
EDSS; median (range)
Time to EDSS 3.0 (years); mean (SD)
median (range) (n59)
Time to EDSS 4.0 (years); mean (SD)
median (range) (n54)
Time to EDSS 6.0 (years); mean 5 median (n51)
MSFC, z score; mean (SD)
Number of GEL; mean (SD)
T2 lesion volume, ml; mean (SD)
16.27 (3.0–57.17)
Prior approved disease-modifying therapy*
3 Glatiramer acetate
Abbreviations: EDSS 5 Expanded Disability Scale Status; GEL 5 gadolinium enhancing lesions; ml 5milliliter; MSFC 5 Multiple sclerosis functional composite; MSSS 5 Multiple Sclerosis Severity Score; SD 5standard deviation. IFN5 interferon beta; *Six patients had received more than one prior multiple sclerosismedication.
(CD19+IL10+) in blood by flow cytometry. Patients treated with MSCs showed anon-significant decrease in the frequency of Th1 population in comparison withplacebo This decrease was maintained along time and persisted overthe subsequent 6 months of placebo treatment, suggesting a carryover effect. Th17population also showed a modest decrease in patients treated with MSCs (Accordingly, Th1/Th17 ratio was decreased in patients treated withMSCs in comparison with placebo. Breg cell frequency showed an increase whenpatients were treated with MSCs in comparison with placebo treatment, even if thepercentage of Breg respect to the total B population in MSCs treated patients wasdecreased ). We did not found differences regarding natural Tregand induced Treg populations (). To avoid the possible carryovereffect we also compared the results between patients treated with MSCs and treatedwith placebo during the first period (, MSCs1 and P1), and we confirmed
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
Figure 2. Relapses and gadolinium-enhancing lesions during the study. Abbreviations: GEL 5 gadolinium-enhancing lesions; MSCs 5 mesenchymalstem cells; NA 5 not available; Scr 5 screening.
the non-significant reduced frequency of Th1 cells. Finally, we compared theimmunological profile of the patients treated with MSCs freshly infused in the firstperiod (, MSCs1) and those treated with cryopreserved MSCs after 6months MSCs2), and we did not observe significant differences.
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
Table 2. Primary and secondary outcomes.
Placebo period n59
Cumulative number of GEL
Change in the number of GEL 6.8 (6.2)
Number of new or enlarging T2lesions
Change in T2 lesion volume,ml
1.08 (20.029–12.31)
0.025 (20.94–3.18)
Percentage of brain volumechange, %
20.01 (20.68–0.28)
20.5 (21.45–0.34)
Change in RNFL thickness
Change in macular volume
MSFC z-score change
0.27 (20.25–0.93)
aU Mann-Whitney for independent samples.
bWilcoxon's test for paired samples.
cNegative binomial regression adjusted by gadolinium-enhancing lesions at baseline. Abbreviations: GEL 5 gadolinium enhancing lesions; EDSS 5Expanded Disability Status Scale; ml 5 milliliter; MSFC 5 Multiple Sclerosis Functional Composite; OD 5 right eye; OS 5 left eye; RNFL 5 retinal nervefiber layer.
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
Figure 3. Effects of MSCs in T and B cell population frequency in blood. Results are shown as percentages respect to the referring cell population (Th1,Th17, CD19 and Treg) and not referred to the total lymphocyte counts. Treatment with mesenchymal stem cells showed a non-significant decrease of theTh1/Th17 populations, increase in regulatory B cells (B reg) population and no changes regarding natural (Nat T reg) and induced (Ind T reg) regulatory Tcells populations. Percentage of each population is shown in the graphics regarding the type of therapy, placebo (P) or mesenchymal stem cells (MSCs) andperiod of treatment, 1 (first period, from month 0 to month 6) or 2 (second period, from month 6 to 12 months).
Evidence from preclinical studies suggests that MSCs are effective in experimentalmodels of MS and could induce their therapeutic effect through mechanismsother than tissue replacement. In fact, MSCs have prominent immunomodulatoryand immunosuppressive properties The observation in the current study ofa decrease in inflammatory MRI measures along with reduced Th1 proin-flammatory responses would support this notion.
Our trial differed from previous studies in two aspects. First, we recruited a
homogenous cohort of patients with active RRMS who failed to standard
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
therapies to evaluate their effects on inflammatory MRI parameters. In contrast,most of the reported studies were phase I safety trials and included secondaryprogressive MS progressive MS relapsing-remitting and secondaryprogressive MS and active but unspecified MS patients and a phase IIatrial on secondary progressive MS which included clinical (visual) andneurophysiological parameters of efficacy Moreover, in one of them theadministration was intrathecal and 5 of the 15 patients also received additional IVMSCs Second, and more important, this is the first randomized, placebo-controlled trial. Both factors may contribute to answer questions concerning theefficacy of the therapy. However, our study has in common with previous studiesthe small number of patients that were enrolled (median 10, range 6–25). Inagreement with previous reports the trial confirmed that MSCs are safe andtheir administration well tolerated.
Although we did not reach the statistical significance for the primary MRI-
based endpoint, the trend to lower cumulative GEL at 6 months and theconfirmation of GEL reduction at the end of the study support the suggestedimmunomodulatory effect of the MSCs
An unknown issue is how long the biological effect of a single dose lasts. That is
why the primary endpoint was analyzed in two ways, at 6 months to avoid thepossible carryover in the second period, and comparing each patient with him/herself in both periods of therapy. Indeed, our data suggests that the effect can lastmore than 6 months because the cumulative number of GEL was lower in thesecond period than in the first 6-month period. Additional evidence comes fromthe immunological analysis which showed the persistence of decreased Th1population over the subsequent 6 months after MSCs therapy. Although the studywas not designed to evaluate the effect of cryopreservation on the immunologicalfunctions of the cells, the observed effect on the MRI in the second period wouldsupport that the cryopreservation does not negatively affects the properties of theMSCs In fact, we did not find significant differences in the immunologicalprofile of the patients treated with MSCs freshly infused or after cryopreservation.
This is the first longitudinal immunomodulatory data in MS on MSCs
treatment We observed immunological changes that were consistentwith a lower proinflammatoty T cell profile, resulting from the decrease in theproportion of IFN-c and with lesser intensity of IL-17-producing CD4+ T cells,and a reduced Th1/Th17 ratio that could explain in part the MRI results we foundconsidering that Th1 and Th17 responses have been linked to disease activity In contrast, we did not find changes in the frequency of cells associated withimmune regulatory function Given the high variability of immunological data(and the restricted sample size we would have been able to detect onlyvery strong effects which was not the case. It would also be of interest to analyzechanges in antigen-specific cell frequency or function.
It is important to acknowledge the difficulties of conducting a placebo-
controlled trial in very active RRMS patients, and patient 1 is one example.
However, it allows identifying as regression to the mean what could bemisinterpreted as therapeutic effect in uncontrolled studies. For ex. four patients
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
did not have any relapse during the trial although they had had a median of 1.5relapses in the previous year.
Although the apparent benefit based on the effect on GEL, a surrogate marker
of disease activity, we did not identify significant differences in other clinical,several quantitative MRI metrics and OCT outcome measures that could beinformative on the possible neuroprotective role of MSCs in addition to theshowed anti-inflammatory effect. The limited number of patients included andthe crossover design of the study may explain part of the lack of beneficial effectsin these measures. Despite these limitations, our data provides justification forfurther clinical testing
Supporting Information
Table S1. List of antibodies for immunological evaluation.
(DOC)
Table S2. MRI secondary endpoints.
(DOC)
Table S3. Evolution of gadolinium enhancing lesions.
(DOCX)
Appendix S1. MRI protocol and Immunological evaluation.
(DOC)
Checklist S1. CONSORT checklist.
(DOC)
Database S1. Main clinical trial database.
(XLS)
Database S2. T2-weighted lesion volume database.
(XLS)
Database S3. Magnetization transfer database.
(XLS)
Protocol S1. Trial protocol. Summary of trial protocol design.
(DOC)
Protocol S2. Trial protocol. Trial protocol EudraCT: 2009-016442-74.
(PDF)
The authors thank Dr. M Teresa Anglada (Service of Anesthesia, Hospital Clinic),Dr. Teresa Pujol (Service of Radiology, Hospital Clinic), Dr. E. Munteis (Serviceof Neurology, Hospital del Mar), Dr. A. Cano (Service of Neurology, Hospital deMataro´), Dr. A. Escartı´n (Service of Neurology, Hospital de Sant Pau), Dr. IBonaventura (Service of Neurology, Mu´tua de Terrrasa), Dr. N. Bargallo´
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
(Plataforma d'Imatge Me dica IDIBAPS), Elena Fraga-Pumar (IDIBAPS) and SaraVarea (Clinical Trials Unit, Hospital Clinic) for their support.
Author ContributionsConceived and designed the experiments: SL MS YB PM BM JB IG EMH NSVJAA BF SB BSD FG PV AS. Performed the experiments: SL MS YB BM JB IGEMH NSV EJA BF SB BSD PV AS. Analyzed the data: SL MS YB BM IG EMHNSV EJA BF SB FG PV AS. Contributed reagents/materials/analysis tools: SL MSYB PM BM JB IG EMH NSV JAA EJA BF SB BSD. Wrote the paper: SL MS YBPM BM JB IG EMH NSV JAA EJA BF SB BSD FG PV AS.
Uccelli A, Laroni A, Freedman MS (2011) Mesenchymal stem cells for the treatment of multiplesclerosis and other neurological diseases. Lancet Neurol 10: 649–656.
Rice CM, Kemp K, Wilkins A, Scolding NJ (2013) Cell therapy for multiple sclerosis: an evolvingconcept with implications for other neurodegenerative diseases. Lancet 382: 1204–1213.
Karussis D, Karageorgiou C, Vaknin-Dembinsky A, Gowda-Kurkalli B, Gomori JM, et al. (2010)Safety and immunological effects of mesenchymal stem cell transplantation in patients with multiplesclerosis and amyotrophic lateral sclerosis. Arch Neurol 67: 1187–1194.
Yamout B, Hourani R, Salti H, Barada W, El-Hajj T, et al. (2010) Bone marrow mesenchymal stem celltransplantation in patients with multiple sclerosis: a pilot study. J Neuroimmunol 227: 185–189.
Rice CM, Mallam EA, Whone AL, Walsh P, Brooks DJ, et al. (2010) Safety and feasibility ofautologous bone marrow cellular therapy in relapsing-progressive multiple sclerosis. Clin PharmacolTher 87: 679–685.
Bonab MM, Sahraian MA, Aghsaie A, Karvigh SA, Hosseinian SM, et al. (2012) Autologousmesenchymal stem cell therapy in progressive multiple sclerosis: an open label study. Curr Stem CellRes Ther 7: 407–414.
Connick P, Kolappan M, Crawley C, Webber DJ, Patani R, et al. (2012) Autologous mesenchymalstem cells for the treatment of secondary progressive multiple sclerosis: an open-label phase 2a proof-of-concept study. Lancet Neurol 11: 150–156.
Freedman MS, Bar-Or A, Atkins HL, Karussis D, Frassoni F, et al. (2010) The therapeutic potential ofmesenchymal stem cell transplantation as a treatment for multiple sclerosis: consensus report of theInternational MSCT Study Group. Mult Scler 16: 503–510.
Kurtzke JF (1983) Rating neurologic impairment in multiple sclerosis: an expanded disability statusscale (EDSS). Neurology 33: 1444–1452.
10. Rudick R, Antel J, Confavreux C, Cutter G, Ellison G, et al. (1997) Recommendations from the
National Multiple Sclerosis Society Clinical Outcomes Assessment Task Force. Ann Neurol 42: 379–382.
Gabilondo I, Martinez-Lapiscina EH, Martinez-Heras E, Fraga-Pumar E, Llufriu S, et al. (2014)Trans-synaptic axonal degeneration in the visual pathway in multiple sclerosis. Ann Neurol 75: 98–107.
12. Velez de Mendizabal N, Hutmacher MM, Troconiz IF, Goni J, Villoslada P, et al. (2013) Predicting
relapsing-remitting dynamics in multiple sclerosis using discrete distribution models: a populationapproach. PLoS One 8: e73361.
13. Francois M, Copland IB, Yuan S, Romieu-Mourez R, Waller EK, et al. (2012) Cryopreserved
mesenchymal stromal cells display impaired immunosuppressive properties as a result of heat-shockresponse and impaired interferon-gamma licensing. Cytotherapy 14: 147–152.
14. Darlington PJ, Boivin MN, Renoux C, Francois M, Galipeau J, et al. (2010) Reciprocal Th1 and Th17
regulation by mesenchymal stem cells: Implication for multiple sclerosis. Ann Neurol 68: 540–545.
PLOS ONE DOI:10.1371/journal.pone.0113936
Mesenchymal Stem Cells in MS
15. Hedegaard CJ, Krakauer M, Bendtzen K, Lund H, Sellebjerg F, et al. (2008) T helper cell type 1 (Th1),
Th2 and Th17 responses to myelin basic protein and disease activity in multiple sclerosis. Immunology125: 161–169.
16. Murphy AC, Lalor SJ, Lynch MA, Mills KH (2010) Infiltration of Th1 and Th17 cells and activation of
microglia in the CNS during the course of experimental autoimmune encephalomyelitis. Brain BehavImmun 24: 641–651.
17. Bland JM, Altman DG (1994) Regression towards the mean. BMJ 308: 1499.
18. Barkhof F, Calabresi PA, Miller DH, Reingold SC (2009) Imaging outcomes for neuroprotection and
repair in multiple sclerosis trials. Nat Rev Neurol 5: 256–266.
PLOS ONE DOI:10.1371/journal.pone.0113936
Source: http://terapiekomorkowe.pl/wp-content/uploads/2016/08/2014-Lliufriu-Randomized-placebo-controlled-phase-II-trial-of-autologous-mesenchymal-stem-cells-in-multiple-sclerosis.pdf
Case-Report Facialisparese Das Krankheitsbild: Periphere Fazialisparese Anatomie: Von seinem Kerngebiet im Hirnstamm zieht der Gesichtsnerv durch den inneren Gehörgang in Nach-barschaft zum VIII. Hirnnerven nach lateral und durchläuft in einem geschwungenen Weg, eingebet-tet in seinen knöchernen Kanal, das Felsenbein. Im Bereich des Mittelohrs verlassen ihn sekretorische (Tränen- und Speicheldrüsen), gustatorische (vordere zwei Drittel der Zunge) und motorische (Stapediusmuskel) Abgänge. Nach Austritt aus dem Foramen styloideum zieht er in die Parotis und teilt sich dort im Pes anserinus in die Äste zur mimi-schen Gesichtsmuskulatur auf. Eine grobe Einteilung unterscheidet die fünf Hauptäste: der Zervi-kalast zum Platysma, der Ramus marginalis mandibulae zum Mund, der Bukkalast, der Augen- und der Stirnast (18).
Biochemical Systematics and Ecology 30 (2002) 837–854 Phytochemical variation within populations of Echinacea angustifolia (Asteraceae) Shannon E. Binns a, John T. Arnason a,∗, Bernard R. Baum b a Biology Department, University of Ottawa, 30 Marie Curie St., Ottawa, ON K1N 6N5, Canada b Eastern Cereal and Oilseed Research Centre, Agriculture and AgriFood Canada,