Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Physiotherapy.org.nz
INVITED CLINICAL COMMENTARY
Sexual wellbeing for people with chronic obstructive pulmonary
disease: relevance and roles for physiotherapy
William MM Levack
PhD MHealSc(Rehabilitation) BPthy
Associate Dean Research & Postgraduate Studies; Senior Lecturer in Rehabilitation
Rehabilitation Teaching and Research Unit, Department of Medicine, University of Otago Wellington, New Zealand
Chronic obstructive pulmonary disease (COPD) is the fifth leading cause of disability worldwide. The purpose of this article is to provide an overview of current knowledge on sexual wellbeing in people with COPD, with particular attention to the possible role of physiotherapy in helping address problems with sexuality resulting from the condition. People with COPD experience more sexual problems on average than the general population, with these issues arising from hormonal, physiological, psychological, sociological and pharmaceutical factors. Physiotherapists can provide specialist support for people with COPD regarding their sex lives through the provision of exercise therapy, advice on positioning to maximise breathing efficacy and minimise energy expenditure during sexual activity and via patient education on chronic condition management. The PLISSIT model provides a robust framework for helping physiotherapists clarify their scope of practice when engaging with people who have COPD on matters to do with sexuality. Regardless of age or severity of symptoms, people with COPD are capable of leading full and satisfying sex lives should they wish to do so. Physiotherapists can contribute information and solutions to support them in this endeavour.
Levack WMM (2014) Sexual wellbeing for people with chronic obstructive pulmonary disease: relevance and roles for physiotherapy New Zealand Journal of Physiotherapy 42(2): 170-176.
Key words: Pulmonary disease, Chronic obstructive; Sexuality; Sexual dysfunction; Dyspnoea; Exercise
people (Collins et al 2012, Fletcher and Martin 1982, Kahraman et al 2013, Kaptein et al 2008, Karadag et al 2007, Köseo˘glu et al
Sex is an important part of life, self-identity and general
2005, Schönhofer et al 2001, Schouten et al 2007) but as noted
wellbeing for the majority of people. It is well established
above there appears to be very little experimental research into
that many adults maintain sexually active lives well into their
strategies to help people with COPD deal with issues related to their
older years (Lindau et al 2007, Matthias et al 1997, Nicolosi et
sexual wellbeing.
al 2004). While sexual activity and sexual interest do tend to decline with age, even very elderly people can enjoy sex and
The purpose of this paper, therefore, is to provide an overview
include it as part of their intimate relationships. One relatively
of current knowledge on sexual dysfunction and sexual health
recent US study found that 38.5% of men and 16.7% of
in people with COPD, with particular attention to the possible
women in the 75-85 year old age group had participated in
role of physiotherapy in helping people with COPD maintain or
sexual activity with a partner in the previous year, with 54% of
regain an active and enjoyable sex life should they choose to
those who were sexually active engaging in sexual activity more
do so. It is argued within this paper that physiotherapy has the
than two or three times a month (Lindau et al 2007).
potential to make a unique contribution to this area of clinical practice because of expertise in chronic condition management,
At all ages, however, sexual activity and sexual satisfaction is
exercise conditioning and use of positioning to enhance the
negatively influenced by poorer health status (Lindau et al 2007,
efficiency of breathing in people with COPD.
Matthias et al 1997). This has been the subject of a body of research, guidelines and systematic reviews for a number of
Definitions and assumptions
conditions including cardiovascular disease (eg Steinke et al 2013),
Sexual activity should be considered a broad term referring to a
diabetes (eg Pontiroli et al 2013, Vardi and Nini 2007), and cancer
wide range of personal interactions and behaviours including,
(eg Miles et al 2007). Arguably less research or clinical guidelines
but not limited to, sexual intercourse. For the purposes of
have been published on the topic of sexual health for people
this paper, a modified version of a definition promoted by
with chronic obstructive pulmonary disease (COPD). In preparing
Lindau et al (2007) will be used: specifically, the term ‘sexual
this paper, only one randomised controlled trial (Svartberg et al
activity' (to be considered synonymous with ‘sex') will be
2004) and no systematic reviews were identified on the topic of
used to refer to ‘any mutually voluntary activity with another
management of sexual dysfunction for people with COPD. This
person that involves sexual contact, whether or not intercourse
is significant because, according the World Health Organizations'
or orgasm occurs or any solitary sexual self-stimulation for
Global Burden of Disease study, COPD is currently the 5th ranked
pleasure'. Neutral terminology has been used throughout
cause of years with disability worldwide (Vos et al 2013) – a more
this paper regarding sexual orientation, except in situations
significant contributor to years with disability in fact than ischaemic
describing research studies that specified the gender of people
heart disease (ranked 21st), diabetes (ranked 9th) or all cancers
in relationships under investigation. Specific issues relating
(ranked below 25th). Furthermore, there is growing evidence that
to transgender people, however, are outside the scope of this
COPD is frequently associated with sexual dysfunction for many
paper due to restrictions on article length.
170 NEW ZEALAND JOURNAL OF PHYSIOTHERAPY
Prevalence of sexual dysfunction in people with COPD:
with self-esteem influencing sexual activity or problems with
The majority of empirical research on sex and COPD to date
general sexual satisfaction (Kaptein et al 2008). However, given
has focused on the prevalence of sexual dysfunction in COPD
the very small sample size, it is highly questionable whether this
populations. Sexual dysfunction can include problems with erectile
study was sufficiently powered to detect such differences if they
dysfunction or premature ejaculation in men; difficulties with vaginal
lubrication for women; or lack of interest in sex, inability to achieve
One additional study has investigated sex behaviour and sexual
orgasm, pain during sex, anxiety about performance or sex not
functioning in 383 men and women who used noninvasive
being pleasurable for either men or women.
mechanical ventilation in the home. This study combined
In men with COPD, erectile dysfunction (i.e. difficulty getting
findings from people with COPD (45% of the total study
or maintaining an erection) has been identified as one of the
population; 173/383) with those who had chronic respiratory
most common problems with sexual performance. Estimates
failure due to other causes (Schönhofer et al 2001). Thirty-four
of prevalence of erectile dysfunction in men with moderate to
percent of these respondents reported being sexually active
very severe COPD have ranged from 72% to 87% (Collins et al
and 61% were not (5% did not answer this question). Sexually
2012, Kahraman et al 2013, Karadag et al 2007, Köseo˘glu et
active people were more likely have better lung function (higher
al 2005). This can be compared to a prevalence of 9-22% for
vital capacity, better force vital capacity, and higher partial
erectile dysfunction that has been reported in the 50-70 year
pressure of oxygen in arterial blood at rest), were more likely
old age group in a large, international, population-based study
to be married or have a partner and were more often younger.
of sexual dysfunction (Laumann et al 2004, Nicolosi et al 2004).
However, no statistically significant differences were noted
Some of these differences in reported prevalence could be
between men and women in this study; both groups were
explained by differences in the categorisation and measurement
equally likely to be sexually active at all ages.
of erectile dysfunction. However, studies which have compared
Notably, in this study, while older people were less likely to be
men with COPD against age-matched controls (using the
sexually active, 20% of those over 70 years on noninvasive
same measurement tool for both) have also found significant
mechanical ventilation still reported continuing to have an
differences in prevalence between these groups. Kahraman
active sex life (Schönhofer et al 2001). Furthermore, while
et al (2013) found varying degrees of erectile dysfunction in
36% of respondents reported a decrease in their sexual activity
79% of 70 men with COPD in comparison to 56% of 68 age-
after initiating home-based mechanical ventilation, 12.6%
matched controls, with men who had COPD generally reporting
of respondents reported their sexual activity had increased as
more severe problems. Similarly, comparing 95 men with stable
a result of the introduction of ventilatory support. In other
moderate-to-severe COPD to 30 age-matched controls, Karadag
words, it is a mistake to assume age or severity of respiratory
et al (2007) found 21% of those with COPD to have ‘severe'
impairment necessarily limits people's capacity or enthusiasm for
erectile dysfunction and 36% to have ‘moderate' erectile
sexual activity.
dysfunction versus 10% of the controls for both ‘severe' and ‘moderate' erectile dysfunction. Furthermore, in a population-
Returning to the subject of gender differences, it has been
based study of erectile dysfunction in the Netherlands involving
suggested that COPD presents less of a problem for female
975 men aged 50-75, COPD was found to be one of five
sexuality than male sexuality. One view is that male sexual
independent determinants for risk of erectile dysfunction
activity is generally more dependent on health status than
(Schouten et al 2007).
female sexual activity, and that for women, ‘the existence of a sexually interested partner and a pleasurable sexual
In comparison to age matched norms, significantly more men
biography are even more important' (Schönhofer et al 2001,
with COPD have also been found to report reduced sexual
p.1612). Another view has been that male sexuality is more
desire and lower frequency of sexual intimacy; with their
vulnerable to dyspnoea and loss of self-esteem resulting from
sexuality more often negatively influenced by low self-esteem
impaired physical performance (Pietropinto and Arora 1989).
and with an overall lower sense of satisfaction with their sex
However, it is important to note that all of these viewpoints and
lives (Kaptein et al 2008). Collins et al (2012), in a study of 90
perspectives have arisen from expert opinion and anecdote;
men with stable moderate-to-severe COPD, found 74% had at
detailed studies on the effect of COPD on women's sexuality
least one sexual problem. In additional to erectile dysfunction,
have yet to be conducted.
many of these men also reported lack of sexual interest (37%), inability to achieve orgasm (42%), and difficulty with finding
Causes of sexual dysfunction in people with COPD:
sex pleasurable (28%). Furthermore, these issues were most
The interaction of variables contributing to sexual dysfunction in
often described as ‘very much of a problem' or ‘somewhat of a
people with COPD is complex, but broadly speaking problems
problem' for these men (Collins et al, 2012).
can arise from a combination of hormonal, physiological, psychological, sociological and pharmaceutical factors.
In comparison, sexual dysfunction in women with COPD has yet to be investigated in depth. One exception has been a
Hormonal factors
study of sexual dysfunction in people with COPD or asthma,
With respect to hormonal issues, it has been established that
in which ten women with COPD provided information on
men with COPD have lower total testosterone levels than men
their experiences and feelings regarding sexuality and intimate
without COPD. A recent systematic review involving a meta-
relationships (Kaptein et al 2008). This study found that,
analysis of data from nine case control studies found that men
when compared to age-matched controls, women with COPD
with COPD have on average 3.21 nmol/L (95% CI 1.23 to 5.18
reported a significantly lower frequency of sexual intimacy, but
nmol/L) less total testosterone than age-matched men without
no significant differences were reported for other aspect of
COPD (Atlantis et al 2013). Testosterone contributes to muscle
sexuality, eg physical problems reducing sexual desire, problems
mass and the body's response to exercise, but is also directly
NEW ZEALAND JOURNAL OF PHYSIOTHERAPY
171
associated with sexual functioning in men. In Collin et al's
the position and mechanical efficiency of the diaphragm, the
(2012) observational study, adults with COPD who had low free
availability and mechanical efficacy of accessory muscles for
serum testosterone levels were over three times more likely to
breathing, the synchronicity of thoracic and diaphragmatic
have erectile dysfunction than adults with COPD who did not
movements, the energy (and therefore oxygen) required to
have low testosterone levels.
maintain the position, and, particularly significantly, ventilation/perfusion matching (Cavalcanti et al 2014, Dean 1985, Heijdra
et al 1994, Jones et al 2003). Ventilation/perfusion matching
COPD is also of course associated with reduced exercise capacity
refers to the efficiency and adequacy of air in the alveoli
secondary to hypoxaemia, dyspnoea and general physical
(ventilation) reaching lung tissue that is sufficiently serviced
deconditioning. This too can be a reason for problems with
by blood from the pulmonary artery (perfusion). Of note,
sexual functioning (Karadag et al 2007, Schönhofer et al 2001,
the physiological response of individual people with COPD to
Steinke 2013). If a person is becomes too breathless or fatigued
changes in body position can be very idiosyncratic; influenced
during sexual activity, or finds his or her limited exercise capacity
by factors such as degree of hyperinflation, asymmetry in
worrying, embarrassing or disempowering, then difficulties both
lung tissue damage, the presence of sputum in the airways,
with sexual arousal and sexual performance can result. Sexual
distribution of body mass and state of arousal or relaxation.
intercourse is often compared to an exercise workload of 3-4 metabolic equivalents (METS) (Collins et al 2012, Steinke et al
As an illustration of this point, the only observational study to
2013). One MET is defined as the amount of oxygen consumed
date on the effect of sexual activity on gas exchange in the
while sitting at rest: specifically 3.5 ml of oxygen per kg of body
context of COPD (albeit based on a single case study) reported
weight per minute of activity (Jette et al 1990), with 3-4 METS
the unexpected finding that, rather than dropping, oxygen
being equivalent to walking on a treadmill at 5-7 kph (i.e. a
saturation rose during sex, peaking during the 10 minute period
brisk walk). For this reason, in people with heart disease (where
after intercourse (Polverino et al 2008). The ‘case' in this study
concerns can exist regarding the likelihood of sexual activity
was a 63 year old man with severe but stable COPD, engaging
causing a myocardial infarct) individuals are usually advised
in sex in ‘comfortable' positions. The authors of the study
that if they can achieve an energy expenditure of ≥ 3-5 METS
speculated that oxygen saturation may have risen during sex for
on formal exercise testing without exhibiting symptoms of
this man because the positions used (in this case, standing or in
ischaemia, then it should be very safe for them to resume their
the ‘woman-on-top' position) resulted in improved ventilation/
normal sexual activity (Steinke et al 2013).
perfusion matching in comparison to breathing at rest, without significant additional energy expenditure for muscle activity.
One of the original studies that is often cited to justify this figure
However, as noted above, cardiorespiratory responses to body
of 3-4 MET is an observational study involving ten healthy,
position can differ for individual people with COPD, which
married couples, aged 25-43, in which heart rate and oxygen
means that sex positions that work for one couple may not
consumption were measured during sexual intercourse (Bohlen
be suitable for another. Individual assessment of physiological
et al 1984). In fact, in this study, physiological responses were
response to different body positions may be warranted.
recorded only for the male partner, and the figure of 3-4 METs was only achieved during the penetration and orgasm stages
Psychological and sociological factors
of sex if using the ‘man-on-top' position for intercourse. Other
In addition to physiological consequences of lung disease, COPD
types of sexual activities, however, were associated with lower
is also associated with psychological and sociological responses
maximum energy expenditure: an average of 1.4 METs (95%
which can negatively influence sexual interest, arousal and
CI 1.2 to 1.6 METs) during foreplay; 1.7 METs (95% CI 1.3 to
behaviour. Collins et al (2012), for instance, suggested that
2.1 METs) during orgasm when the woman was stimulating the
physical limitations arising from COPD may make men take a
man without intercourse; 1.8 METs (95% CI 1.5 to 2.1 METs)
much more passive approach to sexuality or to avoid sexual
during orgasm when the man was stimulating himself without
activity altogether. They also reported that, despite continuing
intercourse, and 2.5 METs (95% CI 1.8 to 3.1 METs) when
to desire an active sex life, the most commonly perceived
having intercourse in the ‘woman-on-top' position (Bohlen et al
reasons for decreased sexual activity among the 90 men with
1984) 1. The figure of 3-4 METs therefore is conservatively high,
COPD in their study was the participants' belief that they were
appropriate to use perhaps when advising people about risk of
‘too old' or ‘too sick'. For both men and women, symptoms
myocardial infarct, during sex, but potentially misrepresentative
of COPD such as breathlessness, coughing and sputum can
of the level of exercise capacity that is necessarily required for
contribute to feeling unattractive and to loss of self-esteem,
an enjoyable sexual encounter. For this reason, de Araújo (2009)
which can affect both attitudes towards sex and physical
has suggested that instead of using the analogue of a ‘brisk
responses during it (Steinke 2013). Fear and anxiety about
walk', sexual activity could be more usefully compared to ‘a
dyspnoea can result in stress associated with sexual activity,
relaxed walk for a few blocks, interspaced by ascending one or
reducing enjoyment and willingness to participate in it (Steinke
two flights of stairs at moderate and, most importantly, at a very
2013). Mood disorders such as depression, which are known
much individual pace' (p.1034).
to be significantly more of a problem for people with COPD than the general population (Di Marco et al 2006, Schneider
Along with exercise deconditioning, people with COPD are
et al 2010), can also negative impact on sexual desire and
also more vulnerable to changes in oxygenation as a result of
changes in body position. In COPD, the position of the body (eg supine lying, prone lying, sitting or standing) can influence
Furthermore, changes in a person's physical body and sexual performance often require couples to develop a renewed
1 Average METs and 95% CI were calculated from the means and standard
understanding of their sexual roles and relationship. This
deviations for oxygen consumption (VO ) for sexual activity reported in Bohlen et al
requires open, honest and caring communication. If either
(1984), using the conversion value of 1 MET to 3.5mL/min/kg VO .
172 NEW ZEALAND JOURNAL OF PHYSIOTHERAPY
or both partners within a couple are unable or unwilling to
discussing sexual matters with the type and extent of involvement in
discuss such matters, sexual wellbeing can suffer. In one unique
interventions for addressing sexual health needs.
study of COPD and intimate relationships, Ibáñez et al (2001)
Within this model, ‘permission' refers simply to letting patients
interviewed 49 men with severe COPD and their partners (all
and their partners be aware that it is perfectly acceptable and
female) separately but concurrently. Sixty-seven percent of the
appropriate to raise questions or express concerns regarding
men reported some type of sexual dysfunction, mostly involving
issues to do with sexuality. This can be done overtly or
less-than-preferred sexual desire or erectile dysfunction; while
covertly. Indirect methods for giving permission might include
94% of their female partners reported noticing changes in the
having information brochures on sexual health and COPD
men's sexual behaviour. Thirty-three percent of the women
visible and accessible in waiting rooms or clinic areas. Direct
also reported that they had noticed negative changes in their
methods might include validating sexuality as a legitimate
partners' communication levels since the onset of COPD and/
topic for discussion if it should arise during clinical interaction,
or home oxygen use, with the women who reported such
or by specifically inviting people to raise it for discussion. For
communication problems being significantly more likely to be
example, if a patient were to make a half-joking reference
dissatisfied in their partners in general than those who did not.
to ‘problems in the bedroom' when discussing respiratory
Of note, fear of causing an exacerbation in their husband's
symptoms, the physiotherapist could respond by saying: ‘yes,
condition appeared to have resulted in over a third of the
sexual function is something that can be affected by COPD, and
women reducing their willingness to engage in sexual activity in
this might be something you would like to discuss further with
this study population.
me or your general practitioner (GP)'.
Giving a person permission to raise issues to do with sexual
Outside the scope of physiotherapy, but still important to know
function does not mean that physiotherapists are then required
about, is the influence of pharmaceuticals on sexual functioning.
to address those issues in full by themselves. If the subsequent
A number of drugs can contribute to sexual dysfunction in both
issues raised are more specific than the physiotherapist is able
men and women. Medications commonly known to reduce
to deal with, a suitable response would be to say: ‘Yes, that is a
sexual desire or sexual performance include diuretics and beta-
valid concern. However, what you are discussing is outside of my
blockers for high blood pressure; anti-depressant, anti-anxiety,
particular training. Would you like me to raise this in a referral
and anti-psychotic medication for mental health conditions;
letter to your GP or respiratory consultant?' The potential benefit
anti-epileptic drugs; steroidal medications such as prednisone;
of simply normalising sexuality as a valid topic for discussion in
and some medications for Parkinson's disease and cancer
the health context should not be underestimated.
treatments (Collins et al 2012, Conaglen and Conaglen 2013, Schouten et al 2007). As COPD is frequently associated with
‘Limited information' is the next level of engagement with
co-morbidities, the possibility that people with COPD may be on
patients on matters to do with sexuality. It involves giving general
medications such as these needs to be taken into consideration.
information about sexuality and sexual function, tailoring this
Incorporating sexual wellbeing in physiotherapy for COPD
information to specific health conditions where appropriate. This includes, for instance, providing education on sexuality to groups
Even when physiotherapists agree that sexual function is an
of people as part of a pulmonary rehabilitation programme or
important area of health and wellbeing, making decisions about
providing general information to individuals in a clinical session,
how to include it (if at all) as a subject for clinical intervention or
drawing on standard information brochures or letting people
patient education can be difficult. Like all health professionals,
know about other clinical or information services relevant to
physiotherapists can feel poorly equipped to address sexuality in
sexuality that are available to them.
clinical practice, can have concerns about making their clients uncomfortable or feel uncertain about the ethical implications
Providing limited information stops short of discussing individual
associated with broaching the topic of sex in the clinic or hospital.
people's actual sex life and instead couches sex interventions within the context of general information that has been helpful
One useful framework for guiding health professionals when
for many people in similar kinds of situations. Within the context
integrating interventions for sexual wellbeing into regular practice
of an interprofessional team it is usually ideal that all team
is the PLISSIT model. Originally proposed as a guide for sex
members are sufficiently comfortable with the topic of sexual
therapists in the 1970's (Annon 1976), the PLISSIT model has
health, and with their own sexuality, to work with any patients
subsequently been applied in a range of different health contexts
at the ‘permission' and ‘limited information' level of the PLISSIT
(Jaarsma et al 2010, Marsden and Botell 2010, McBride and
model (Sipski and Alexander 1997).
Rines 1999, McLeod and Hamilton 2012). It has been promoted as a model appropriate for interprofessional teams (Dunn 1997),
At the ‘specific suggestion' stage of the PLISSIT model,
and already been used in at least one New Zealand rehabilitation
assessment of issues and provision of interventions occurs at
service for this purpose (Simpson et al 2006).
the individual patient level. In terms of physiotherapy, this might including making recommendations regarding positioning
PLISSIT is a mnemonic which stands for permission (P), limited
to minimise dyspnoea and maximise body movements with
information (LI), specific suggestions (SS), and intensive therapy
minimum energy expenditure during sex. It might also involve
(IT). These four terms relate to four levels of engagement that a
advice regarding management of home oxygen and ventilators
health professional can take with any client when considering the
to support sexual activity. Generally speaking, this level
topic of sexual functioning and wellbeing. They also correspond
of engagement with patients and their partners is likely to
to increasing levels of intimacy when discussing sexuality in the
require some degree of postgraduate training and should be
clinical setting and so can be used to align a health professional's
accompanied by close professional supervision.
level of training, scope of practice and degree of comfort in
NEW ZEALAND JOURNAL OF PHYSIOTHERAPY
173
The ‘intensive therapy' level of the PLISSIT model refers to
chest, or prolonged activities involving the mouth (eg prolonged
the type of professional input that is usually only provided by
kissing or giving oral sex). Figure 1 provides examples of some
trained relationship counsellors, sex therapists, or physicians. It
sexual positions that have been reported to be effective for
might include ‘psychotherapy; intensive or prolonged marital
people with COPD (Polverino et al 2008, Stitik and Benevento
relationship counselling; counselling and therapy for battering,
sexual abuse, or rape; surgical or invasive procedures… or
People with COPD and their partners can be encouraged to
medical management of infertility; childbirth; hormonal
make use of aids to reduce the physical demand of sexual
imbalances; or severe behavioural or psychiatric problems' (Dunn
activity. This includes making use of sex toys such as vibrators
1997, p. 398). As such, this level of engagement with patients
(which can be privately purchased online) as well as medical
and their partners is useful to know about, but is generally
devices to reduce the work of breathing. If using supplementary
outside the scope of practice of physiotherapists, except for a
oxygen or ventilators at home, people with COPD should be
few specific topics within specialist areas (eg perhaps within
encourage to use these during sex too, adjusting ventilators
women's health physiotherapy).
settings to compensate for increased breath frequency and tidal
Interventions for sexual dysfunction for people with COPD:
volumes within comfortable limits (Schönhofer et al 2001).
For the purpose of this paper, interventions for sexual
Outside the scope of physiotherapy are medical interventions to
dysfunction can be divided into those that can be provided
compensate for sexual dysfunction. These include, for instance,
by physiotherapists and those which need input from other
the use of phosphodiesterase inhibitors (eg Sildenafil citrate;
specialist health professionals. In terms of physiotherapy,
sold as Viagra), hormonal therapy in the case of hypogonadism
interventions for improving sexual satisfaction for people with
(Svartberg et al 2004), or vacuum pumps and penile implants
COPD might include:
to treat erectile dysfunction (Hackett et al 2008). Psychosexual
Advice on cardiorespiratory training to improve general
counselling, relationship counselling and cognitive behaviour
exercise capacity (with exercise also potentially resulting in
therapy interventions may also be helpful for dealing with
improved mood and self-esteem);
psychological and social issues related to sexual functioning (Steinke 2013), although access to these type of therapies may
Training of people with COPD in sputum clearance techniques
be restricted by cost. While not directly involved in the provision
(eg postural drainage and active cycle of breathing), with
of these interventions, physiotherapists can play a role in raising
advice to use these techniques prior to engaging in sexual
the possibility of them to people with COPD.
activity so as to minimise coughing and maximise lung capacity during sex;
Advice regarding use of bronchodilators, where these have
A pleasurable and satisfying sex life is important to many people
been prescribed, prior to engaging in sexual activity;
with COPD regardless of age or severity of impairments. Factors
Advice regarding fatigue management, including preparing
contributing to problems with sexual functioning are complex
for sexual activity through use of relaxation techniques and by
and interrelated, but in the presence of COPD sexuality can
picking times when feeling well rested;
be affected by hormonal dysfunction, exercise deconditioning, exertional dyspnoea, the psychological and sociological
Assessment and training of people with COPD in the use
consequences of having a chronic condition and by the side-
of positioning to maximise ventilation/perfusion matching,
effects of common medications. Physiotherapy has a role to
maximise capacity for movement with minimum energy
play in the management of problems with sexual function in
expenditure and minimum dyspnoea during sexual activity;
COPD, providing guidance in the restoration of exercise capacity,
Encouraging people with COPD and their partners to talk to
the use of positioning to maximise efficiency of breathing and
one another about their changing bodies, what they find easy
movement and in the everyday management of respiratory
or difficult to do, what they still find pleasurable and enjoyable
and to explore new ways of physically interacting with one another for pleasure;
KEY POINTS
Reminding people the full range of sexual activities that are
• A pleasurable and satisfying sex life is important to
open to them, reinforcing the notion that sexual activity is not
many people with COPD regardless of age or severity of
just limited to intercourse, but can involve other activities too,
such as kissing, cuddling and touching (activities which are not
• COPD can have a negative influence on sexuality due
only enjoyable in themselves, but which can also be a good
to hormonal, physiological, psychological and social
way of building up tolerance for other activities in the future).
consequences of the disease.
In terms of positioning for sexual intercourse, there are a
• Physiotherapy can play an important role in helping people
number of factors likely to contribute to increased dyspnoea
with COPD and their partners deal with issues to do with
for people with COPD and so should be avoided, particularly if
respiratory symptoms are severe. These include lying completely
• The PLISSIT model provides a framework to help
flat in supine, being in a position that requires high levels of
physiotherapists decide what level of involvement they
energy expenditure to maintain (eg sustaining a prone lying
should have regarding interventions for improving a person's
position, propped up on arms, such as when lying on top of
sexual wellbeing.
one's partner), having a weight (eg one's partner) on one's
174 NEW ZEALAND JOURNAL OF PHYSIOTHERAPY

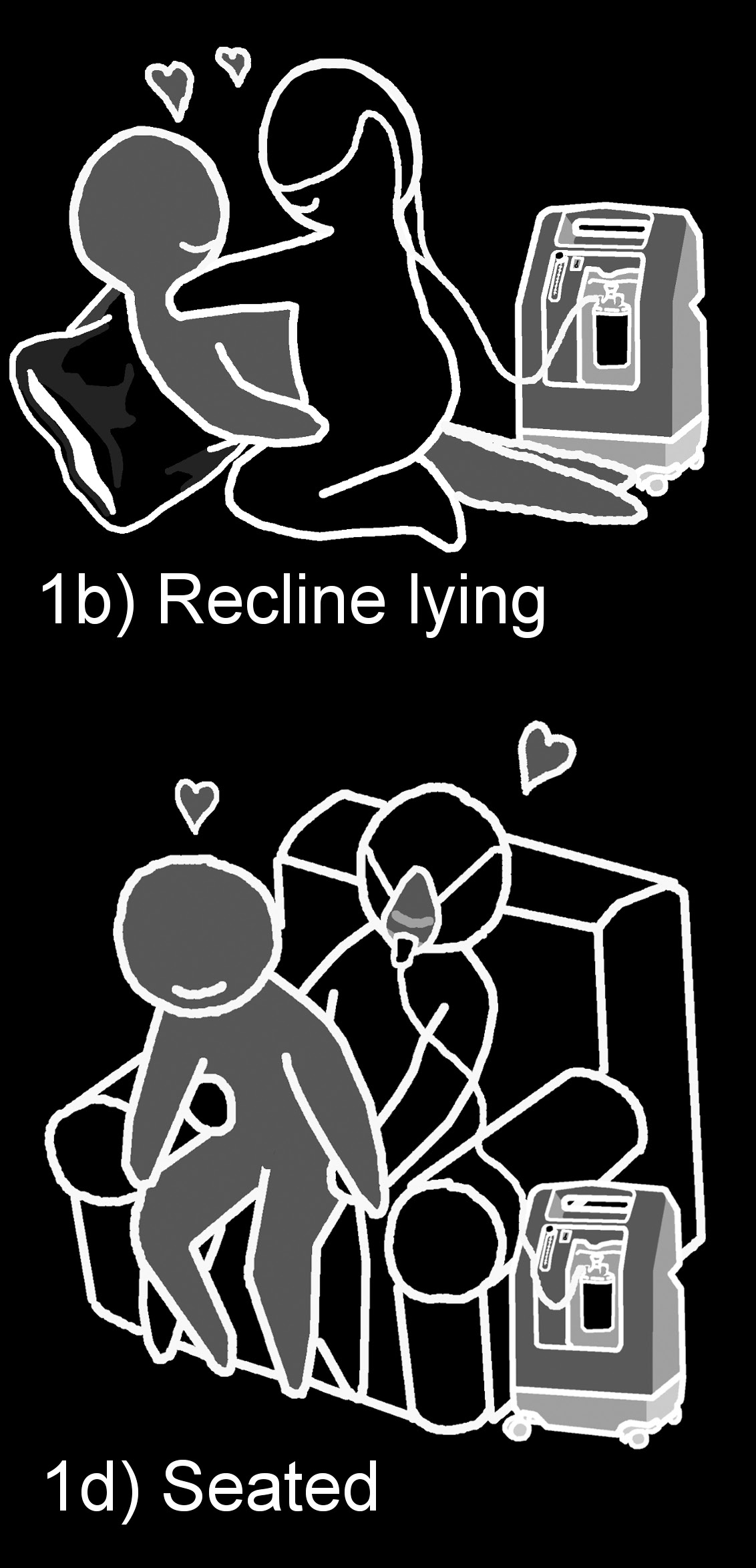
Figure 1: Sex positions for people with COPD and their partners
Figures 1a-1d provide examples of sex positions reported to be effective for people with COPD. While only one of the partners in these illustrations is presented as having COPD, these positions are suitable if either partner has COPD. People with COPD should be encouraged to make use of pillows during sex for comfort, to elevate parts of the body and to support limbs.
Figure 1a: Side lying
Figure 1b: Recline lying
Figure 1c: Standing
Figure 1d: Seated
ADDRESS FOR CORRESPONDENCE
Atlantis E, Fahey P, Cochrane B, Wittert G, Smith S (2013) Endogenous
testosterone level and testosterone supplementation therapy in chronic
William Levack, Department of Medicine, University of Otago
obstructive pulmonary disease (COPD): A systematic review and meta-
Wellington, PO Box 7242, Wellington 6242. Phone: +64 4 918
analysis. BMJ Open 3: e003127.
6279. Email: [email protected]
Bohlen JG, Held JP, Sanderson MO, Patterson RP (1984) Heart rate, rate-
pressure product, and oxygen uptake during four sexual activities.
Archives of Internal Medicine 144: 1745-1748.
Cavalcanti ABL, Rattes Lima CSF, Barros de Sá R, Reinaux CMA, Braz Júnior
Annon JS (1976) The PLISSIT model: A proposed conceptual scheme for the
DS, Teixeira AL, Dornelas de Andrade A, Marinho PEM (2014) Influence
behavioral treatment of sexual problems. Journal of Sex Education and
of posture on the ventilatory pattern and the thoraco-abdominal
Counseling 2: 1-15.
kinematics of patients with chronic obstructive pulmonary disease (COPD). Physiotherapy Theory and Practice 30: 490-494.
NEW ZEALAND JOURNAL OF PHYSIOTHERAPY 175
Collins EG, Halabi S, Langston M, Schnell T, Tobin MJ, Laghi F (2012) Sexual
McBride KE, Rines B (1999) Sexuality and spinal cord injury: A road map for
dysfunction in men with COPD: impact on quality of life and survival. Lung
nurses. SCI Nursing 17: 8-13.
190: 545-556.
McLeod DL, Hamilton J (2012) Sex talk and cancer: Who is asking. Canadian
Conaglen HM, Conaglen JV (2013) Drug-induced sexual dysfunction in men
Oncology Nursing Journal 23: 197-207.
and women. Australian Prescriber 36: 42-46.
Miles CL, Candy B, Jones L, Williams R, Tookman A, King M (2007)
de Araújo CGS (2009) Sexual activity: an exercise to prevent cardiovascular
Interventions for sexual dysfunction following treatments for cancer.
morbidity and mortality? Expert Review Cardiovascular Therapy 7: 1033-
Cochrane Database Systematic Reviews 4: CD005540.
Nicolosi A, Laumann EO, Glasser DB, Moreira Jr ED, Paik A, Gingell C (2004)
Dean E (1985) Effect of body position on pulmonary function. Physical
Sexual behavior and sexual dysfunctions after age 40: The global study of
Therapy 65: 613-618.
sexual attitudes and behaviors. Urology 64: 991-997.
Di Marco F, Verga M, Reggente M, Casanova FM, Santus P, Blasi F, Allegra L,
Pietropinto A, Arora A (1989) Chronic pulmonary disease and sexual
Centanni S (2006) Anxiety and depression in COPD patients: The roles of
functioning. Medical Aspects of Human Sexuality 23: 78-82.
gender and disease severity. Respiratory Medicine 100: 1767-1774.
Polverino F, Santoriello C, De Sio V, Ando F, de Blasio F, Polverino M (2008)
Dunn KL (1997) Sexual education and the team approach. In Sipski ML,
Sexual intercourse and respiratory failure. Respiratory Medicine 102: 927-
Alexander CJ (Eds) Sexual Function in People with Disability and Chronic
Illness edn). Gaithersburg, Maryland: Aspen Publishers, Inc., pp 381-402.
Pontiroli AE, Cortelazzi D, Morabito A (2013) Female sexual dysfunction
Fletcher E, Martin R (1982) Sexual dysfunction and erectile impotence in
and biabetes: A systematic review and meta-analysis. Journal of Sexual
chronic obstructive pulmonary disease. Chest 81: 413-421.
Medicine 10: 1044-1051.
Hackett G, Kell P, Ralph D, Dean J, Price D, Speakman M, Wylie K (2008)
Schneider C, Jick SS, Bothner U, Meier CR (2010) COPD and the risk of
British Society for Sexual Medicine guidelines on the management of
depression. Chest 137: 341-347.
erectile dysfunction. Journal of Sexual Medicine 5: 1841-1865.
Schönhofer B, Von Sydow K, Bucher T, Nietsch M, Suchi S, Köhler D, Jones
Heijdra YF, Dekhuijzen PN, Van Herwaarden CL, Folgering HT (1994) Effects
PW (2001) Sexuality in patients with noninvasive mechanical ventilation
of body position, hyperinflation, and blood gas tensions on maximal
due to chronic respiratory failure. American journal of respiratory and
respiratory pressures in patients with chronic obstructive pulmonary
critical care medicine 164: 1612-1617.
disease. Thorax 49: 453-458.
Schouten BWV, Bohnen AM, Dohle GR, Groeneveld FPMJ, Willemsen S,
Ibáñez M, Augilar JJ, Maderal MA, Prats E, Fårrero E, Font A, Escarrabill
Thomas S, Bosch JLHR (2007) Risk factors for deteriorating of erectile
J (2001) Sexuality in chronic respiratory failure: Coincidences and
function: the Krimpten study. International Journal of Andrology 32: 166-
divergences between patients and primary caregiver. Respiratory Medicine
95: 975-979.
Simpson G, Anwar S, Wilson J, Bertapelle T (2006) Improving the
Jaarsma T, Steinke EE, Gianotten WL (2010) Sexual problems in cardiac
rehabilitative management of client sexual health concerns after
patients: How to assess, when to refer. Journal of Cardiovascular Nursing
neurological disability: Evaluation of a staff sexuality training programme in
25: 159-164.
New Zealand. Clinical Rehabilitation 20: 847-859.
Jette M, Sidney K, Blümchen G (1990) Metabolic equivalents (METS) in
Sipski ML, Alexander CJ (1997) Impact of disability or chronic illness on
exercise testing, exercise prescription, and evaluation of functional
sexual function. In Sipski ML, Alexander CJ (Eds) Sexual Function in People
capacity. Clinical cardiology 13: 555-565.
with Disability and Chronic Illness: A Health Professional's Guide edn).
Jones AY, Dean E, Chow CC (2003) Comparison of the oxygen cost of
Gaithersburg, MD: Aspen Publishers, pp 3-12.
breathing exercises and spontaneous breathing in patients with stable
Steinke EE (2013) Sexuality and chronic illness. Journal of gerontological
chronic obstructive pulmonary disease. Physical Therapy 83: 424-431.
nursing 39: 18-27; quiz 28-19.
Kahraman H, Sen B, Koksal N, Kilinç M, Resim S (2013) Erectile dysfunction
Steinke EE, Jaarsma T, Barnason SA, Byrne M, Doherty S, Dougherty CM,
and sex hormone changes in chronic obstructive pulmonary disease
Fridlund B, Kautz DD, Mårtensson J, Mosack V (2013) Sexual counseling
patients. Multidisciplinary respiratory medicine 8: 66.
for individuals with cardiovascular disease and their partners: A consensus
Kaptein AA, van Klink RC, de Kok F, Scharloo M, Snoei L, Broadbent E,
document from the American Heart Association and the ESC Council on
Bel EH, Rabe KF (2008) Sexuality in patients with asthma and COPD.
Cardiovascular Nursing and Allied Professions (CCNAP). Circulation 128:
Respiratory Medicine 102: 198-204.
Karadag F, Ozcan H, Karul AB, Ceylan E, Cildag O (2007) Correlates of
Stitik TP, Benevento BT (1997) Cardiac and pulmonary disease. In Sipski
erectile dysfunction in moderate-to-severe chronic obstructive pulmonary
ML, Alexander CJ (Eds) Sexual Functioning in People with Disability and
disease patients. Respirology 12: 248-253.
Chronic Illness edn). Gaithersburg, Maryland: Aspen Publishers, Inc., pp 303-335.
Köseo˘glu N, Köseo˘glu H, Ceylan E, Cimrin H, Özalevli S, Esen A (2005) Erectile
dysfunction prevalence and sexual function status in patients with chronic
Svartberg J, Aasebø U, Hjalmarsen A, Sundsfjord J, Jorde R (2004)
obstructive pulmonary disease. Journal of Urology 174: 249-252.
Testosterone treatment improves body composition and sexual function in men with COPD, in a 6-month randomized controlled trial. Respiratory
Laumann EO, Nicolosi A, Glasser DB, Paik A, Gingell C, Moreira E, Wang
Medicine 98: 906-913.
T (2004) Sexual problems among women and men aged 40–80 y: prevalence and correlates identified in the Global Study of Sexual Attitudes
Vardi M, Nini A (2007) Phosphodiesterase inhibitors for erectile dysfunction
and Behaviors. International journal of impotence research 17: 39-57.
in patients with diabetes mellitus. Cochrane Database Systematic Reviews 1: CD002187.
Lindau ST, Schumm LP, Laumann EO, Levinson W, O'Muircheartaigh CA,
Waite LJ (2007) A study of sexuality and health among older adults in the
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K,
United States. New England Journal of Medicine 357: 762-774.
Salomon JA, Abdalla S, Aboyans V (2013) Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic
Marsden R, Botell R (2010) Discussing sexuality with patients in a motor
analysis for the Global Burden of Disease Study 2010. The Lancet 380:
neurone disease clinic. Nursing Standard 25: 40-46.
Matthias RE, Lubben JE, Atchison KA, Schweitzer SO (1997) Sexual activity
and satisfaction among very old adults: Results from a community-
dwelling Medicare population survey. The Gerontologist 37: 6-14.
176 NEW ZEALAND JOURNAL OF PHYSIOTHERAPY
Source: http://physiotherapy.org.nz/assets/Professional-dev/Journal/2014-November/new-ICC.pdf
Geophysical Journal International Geophys. J. Int. (2002) 148, 256–277 Morphological dating of cumulative reverse fault scarps: examplesfrom the Gurvan Bogd fault system, Mongolia S. Carretier,1,∗ J-F Ritz,1 J. Jackson2 and A. Bayasgalan21Laboratoire de G´eophysique Tectonique et S´edimentologie, CNRS-UMR, Universit´e Montpellier II, 4, Place Eug ene Bataillon, 34000 Montpellier, France.E-mail: [email protected] Laboratories, Madingley Road, Cambridge, CB3 OEZ England
Journal of Pharmacognosy and Phytochemistry 2013; 2 (3): 55-60 ISSN 2278-4136 Natural Bioenhancers: An overview ISSN 2349-8234 JPP 2013; 2 (3): 55-60 Deepthi V. Tatiraju,* Varsha B. Bagade, Priya J. Karambelkar, Varsha M. Jadhav, © 2013 AkiNik Publications Vilasrao Kadam Received: 19-7-2013 Accepted: 09-8-2013