Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Probram.be
Primary prevention of breast cancer: state of the art in 2012
Fabienne Liebensa*, Birgit Carlya, Pino Cusumanob, Virginie Lienarta, Serge Rozenberga
a ISALA Breast Unit and Prevention Center, OBGYN department, CHU Saint Pierre, Brussels, ULB-VUB. bBreast Unit, CHC Saint Joseph and CHU Sart Tilman, Liège, ULg *Corresponding author: Fabienne Liebens MD, ISALA Breast Unit and Prevention Center, CHU Saint Pierre, 290 rue Haute, 1000 Bruxelles.
Received: 18.09.2012
Accepted: 14.12.2012
Published: xx.04.2013
Abstract
Breast cancer is the most frequent cancer in women and the first cause of mortality linked to malignancies. In
Belgium the mortality rate is 1 on 4 being amongst the highest across EU countries. Despite huge progress in
screening and treatment, cancer remains a plague in the developed world. As a consequence urgent efforts are
needed to foster primary prevention. All women should be encouraged to decrease alcohol consumption, to
control body weight, to exercise, to avoid uncontrolled hormone treatments and to follow healthy lifestyle
thereby reducing cardiovascular risk and diabetes. They should also be informed on the benefits of long lasting
breastfeeding and early pregnancy. More accurate primary prevention allows defining for each woman her
personal risk profile. Indeed undisputed progress has been made nowadays in identifying properly high risk
women likely to benefit from tailored preventive intervention.
Keywords: breast cancer, risk factors, primary prevention
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
Organisation (WHO) defined primary
prevention as "all activities designed to
Cancer is a frequent disease
reduce the instances of an illness in a
affecting one man out of three and one
population and thus to reduce, as far as
woman out of four before age 75 (1). For
possible, the risk of new cases appearing".
the year 2008, 59.996 new malignancies of
According to the European expert group
any type have been diagnosed in Belgium.
for cancer prevention, screening is a
Breast cancer (BC) is the one most
valuable method to limit cancer but as
much as possible primary prevention
representing more than one third of all
should be preferred (4). One also
female cancers. About 9 600 women are
acknowledges that prevention strategies
hit annually, meaning another Belgian
can only be successful if addressing health
woman every hour (2). The mean age of
issues considered being at high risk by the
diagnosis is 61 years. However 25% will
general population. Furthermore validated
occur before age 50. This disease
risk factors should have been identified
represents the first cause of cancer
fatalities in our female population. In 2008,
prerequisites apply to BC.
2 329 deaths were recorded meaning that
A limited proportion of BC (5-
one out of four women still dies from BC.
10%) are linked to genetic predisposition
These unfortunate figures for Belgium
requiring specific diagnostic approaches,
correspond to an annual age standardized
preventive strategies and follow up
incidence rate of 143.6 per 100 000 women
measures. Except this rare situation, the
in contrast to the European average
causes favoring BC are multi-factorial.
fluctuating far lower, closer to 106 (2).
Nevertheless recent advances suggest that
Nonetheless in all developed countries the
a tailored risk pattern should be defined for
number of new cases increases by 1-2%
annually. In 20 years time (1984-2003) the
parameters are quantifiable today and one
incidence has levelled off in some
has to recognize that some of these can be
countries like the United Kingdom
substantially reduced.
reaching 51% (3). BC is also a disease
affecting man: in Belgium about 85 cases
RISK FACTORS LINKED WITH BC
are diagnosed each year.
Despite important progress in
NON MODIFIABLE FACTORS
screening and treatment, BC remains an
epidemiological plague in developed
The incidence of BC varies with
age. Incidences are usually lower in
burden and the financial cost linked to the
women below age 40. Figures increase
treatment of overt disease, important
thereafter and reach their highest values
efforts are urgently needed in the field of
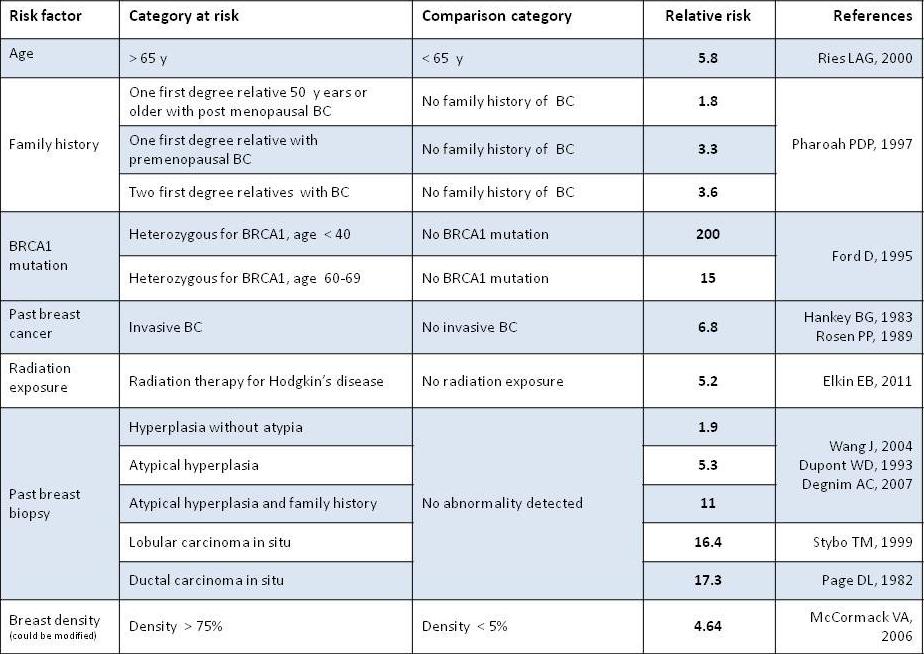
and plateau after 70. A family history
primary prevention. The World Health
influences the level of risk depending on
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
the degree of family relationship with the
without atypia, ductal or lobular atypical
sick parent(s) (mother, sister, daughter),
hyperplasia and in situ cancer. Ductal or
their age at occurrence of the disease and
lobular atypical hyperplasia lesions are
their number (see Table 1). Between 5 and
10% of BC occur in a genetic context and
performed for diagnostic purposes. Their
are transmitted on the autosomal dominant
frequency has increased in the last decade
mode. Namely two different major genes
(6). A personal history of BC also
have been identified; BRCA1 and BCRA2
increases the risk to develop a second
(localized respectively on chromosome 17
cancer in the other breast. Women who
and 13). They account for the majority of
underwent radiation therapy involving
the hereditary cancer forms. Other genes
their breast(s) before the age of 30 are also
also play a role but at a lesser extent
at higher risk. Such situation mostly
(BCRA3, p53, PTEN, ATM). In families
concerns young women irradiated on the
displaying the BCRA1 gene the lifetime
chest for Hodgkin disease.
risk of developing BC before age 70 varies
between 56 and 87%. For ovarian cancer
FACTORS LINKED TO REPRODUC-
the risk ranges between 16 and 60%. A
TIVE LIFE AND HORMONE USE
biopsy finding of an „intra-epithelial
neoplasia‟ (IEN) increases the risk of BC.
Several factors will increase the
Such entities include a number of
risk of BC: early menarche, (relative risk
mammary proliferations like hyperplasia
RR: 1.3; menarche < 12 versus >15 years);
Table 1. Non modifiable risk factors of Breast Cancer (BC)
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
no or late childbearing (RR: 1.7-1.9;
and differentiation. For instance, in
nulliparity or first parity above 30 versus
overweight or obese individuals, an
first parity below 20); late menopause (RR:
increase of several endogenous hormones,
1.2-1.5; menopause above 55 versus before
growth factors and cytokines has been
described. The excess of fat tissue
combining estrogens and progesterone
increases insulin resistance. The resulting
chronic hyperinsulinism facilitates IGF-1
Nevertheless the impact of these factors on
production inducing cell proliferation. On
BC risk remains low. Inversely long lasting
the other hand obesity also induces a
breastfeeding is
protective factor
chronic inflammatory state via increased
(decreased risk of 4, 3% per feeding year)
blood levels of pro-inflammatory factors
facilitating cell proliferation. These pro-
MODIFIABLE FACTORS
interleukin 6 (IL-6), C-reactive protein
(CRP) and leptin. Obesity also induces
research in cancer (IARC) evaluates that
increased blood levels of estrogens
25% of BC are due to overweight and
resulting from the aromatization of
sedentary lifestyle (8). A number of
androgens in fat tissues. The current global
epidemiological surveys indicate that
trends towards a dramatic increase in
women exercising 3-4 hours weekly
overweight and obesity seem to parallel a
decrease their risk by 30-40% compared to
significant decrease in physical activity in
their non-active counterpart. Overweight
the overall population. Such behaviors will
and obese women display an increased risk
after menopause; this increase can be as
incidence (9). For women already suffering
high as 250%, being directly correlated to
from BC one should stress that their way
the weight excess. Alcohol consumption
of life could influence their healing. A
equal or higher than 2 daily glasses also
study exploring the contribution of several
increases the risk both before and after
modifiable risk factors - excluding those
linked to reproductive life - demonstrates
definitively established, some studies
that 21% of BC mortality worldwide can
indicate that diet (rich in animal fat and
be attributed to alcohol consumption,
carbohydrates but low in fruit, vegetables
overweight and lack of physical activity. In
and fibers) could also play a role as a risk
addition, the contribution of modifiable
factors to BC risk in unaffected women is
Several biological mechanisms are
highest in high-income countries (27%)
and the most significant factor is
between modifiable risk factors and BC.
overweight/obesity.
These are mostly mechanisms interfering
intermediate-income
with carcinogenesis via cell proliferation
proportion of BC linked to these risk
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
factors decreases to 18% and exercise is
estrogens and several in vitro studies are
the one contributing most (10%) (11).
currently conducted. Such products are
Finally breast density has been recently
called "endocrine disruptors". Examples
recognized as one of the strongest
independent risk factor of BC apart from
age and genetic mutations (12). Breast
density (BD) is that proportion of breast
polychlorobiphenyls
occupied by radiological dense tissue
released during incineration or burning of
reflecting breast tissue composition. Dense
coal and petrol, bisphenol A (BPA) used in
areas represent fibro glandular, when non
plastic and resins and also parabens
dense areas correspond to fatty tissue.
preservatives used in cosmetics and
Although the mechanisms by which BD
deodorants (14). In the short term it will be
affects BC risk are not well understood, an
impossible to determine with certainty
estimated 16% of all BC have been linked
which role these agents play effectively.
to breast densities higher than 50%. This
implies that among all known BC risk
MODELS ESTIMATING THE RISK
factors BD has the greatest population
OF BREAST CANCER
attributable fraction. Unlike most other risk
factors for BC, BD can be modified by
In recent years important progress
hormonal agents, suggesting that it may be
has been made in identifying women likely
a biomarker for preventive interventions in
to benefit from primary preventive
high risk women (13).
interventions and/or from tailored or
personalized screening approaches. Several
BREAST CANCER AND ENVIRON-
models estimating the risk have been
proposed but none considers all possible
contributing factors. Existing models do
As a concept the environment
not allow predicting with 100% certainty
which woman will or will not develop BC.
biological agents one person will be
Moreover none allows finding out which
exposed to during life. Pesticides, X-rays,
woman will benefit from drug prevention.
electromagnetic fields, cosmetics, cleaning
Nevertheless such tools represent very
agents… The list is long of threatening
valuable means to establish thresholds
agents having a possible link with cancer.
above which preventive therapies can be
Nowadays research is facing in this respect
discussed. Most used models are those
more questions than answers. Indeed any
developed by Gail, Tyrer- Cuzick, Claus,
BCRApro, and Cough (15). Some of these
models make it possible to determine the
challenging to establish. A number of
probability of carrying a BRCA1-2 genetic
chemicals are being investigated since their
mutation. This may be helpful before
biological properties mimic those of
advising genetic testing. Several studies
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
are currently validating the integration of
prevention for unprotected medicinal
BD measurement in the risk appraisal.
products already available as generic
High risk women are those running
a risk between 20-25% or higher to
develop BC during life time or showing a
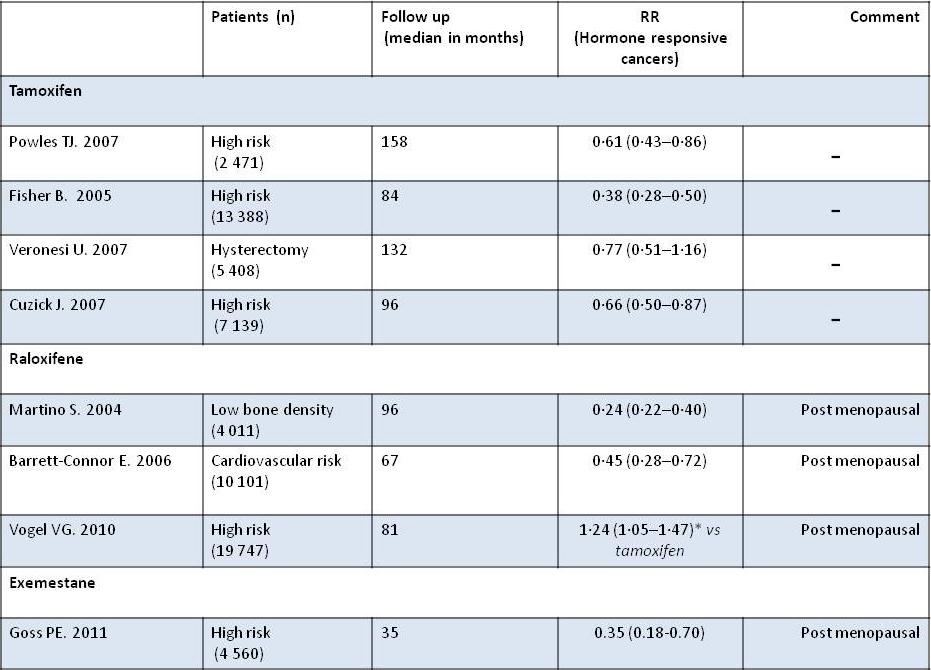
TAMOXIFEN (TABLE 2)
risk between 4-8% at 10 years. One should
remember that the overall risk for any
Tamoxifen is a selective estrogen
woman during her whole life ranges
receptor modulator (SERM). In the
adjuvant setting, patients with hormone
sensitive BC treated with tamoxifen show
PREVENTIVE MEDICATIONS
a 50% risk reduction of contralateral BC.
This finding has led to use tamoxifen for
Based on solid scientific evidence,
primay prevention in high risk women.
three drugs have demonstrated an effect in
Based on four powered double blind
preventing BC in high risk women. These
randomized placebo controlled studies,
drugs are tamoxifen, raloxifene and
tamoxifen (20 mg) given during 5 years
exemestane. Preliminary investigations
has decreased the risk of hormonal
suggest a possible similar effect for
receptor positive BC by 43%. This drug
lasofoxifen and arzoxifen. Promising
does not prevent the occurrence of
malignancies. Tamoxifen also protects
against osteoporosis but increases the risk
Molecules like aspirin or other non steroid
of phlebitis and pulmonary embolism (RR
anti-inflammatory agents, anti COX-2,
1.9 : CI 1.4-2.6), cerebro-vascular bleeding
retinoids and several food supplements
(RR : 1.59) and endometrial cancer (RR :
show limited effect and are in their early
2.4: CI 1.5-4.0). Updates of these studies
development phase (15).
have been recently published and confirm
reimbursed by our social security system
but only for osteoporosis and cardio-
reduction of 38% compared with placebo
vascular diseases. Such possibility is
after 6-10 years of surveillance). Moreover
currently not foreseen for BC. In the US,
side-effects decrease after stopping the
FDA has granted a preventive indication
therapy (15). One can define cohorts of
for tamoxifen and raloxifene. In contrast,
women in which the advantage of drug
in Europe such preventive indication has
prevention will outweigh the risk of drug
not been agreed. It seems very unlikely
(thrombo-embolism,
that the current situation will evolve. Big
cancer). Such women are those displaying
Pharma does not see any financial
atypical hyperplasia or in situ malignancies
advantage in extending the indication to
and particularly if they are premenopausal.
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
Table 2. Summary of the main BC prevention studies
For postmenopausal women the benefit is
effect, low incidence of thrombo-embolic
highest if the risk of endometrial cancer is
events) suggests that it could represent the
discarded (e.g women having undergone
first choice for postmenopausal high risk
RALOXIFENE (TABLE 2)
EXEMESTANE (TABLE 2)
Exemestane belongs to the groups
investigated in the preventive setting in 3
of aromatase inhibitors, the enzyme
studies (Table 2). In two trials the
metabolizing androgens in estrogens in
medication was tested in a group of women
several target organs including breast. In
at high risk of developing diseases other
adjuvant setting for women suffering from
than cancer (cardio-vascular disease or
BC, this therapeutic class seems more
osteoporosis). In the third study, raloxifene
effective than tamoxifen in reducing the
and tamoxifen were compared head to
risk of developing contralateral BC (15).
head in women at high risk of BC. The risk
These aromatase inhibitors do not cause
decreased by 23% and by 38% in the
the gynaecologic or thrombo-embolic
raloxifene group and the tamoxifen group
effects seen with tamoxifen. However they
respectively. This difference was not
increase the risk of bone fracture,
statistically significant. The lowest toxicity
arthralgia and possibly cardio-vascular
profile of raloxifene (no endometrial
events. Exemestane has recently shown its
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
preventive efficacy in post menopausal
women attending our Breast Unit (Liebens
women included in a large double blind
F et al. Abstract 129, 8th European Breast
randomized placebo controlled study. A
Cancer Conference 2012). Most of these
65% reduction of hormone receptor
women belong to the high income
positive BC was demonstrated after a
median follow up of 3 years (RR: 0.35;
recruitment bias, their knowledge of their
95% CI 0.18-0.70). Another aromatase
risk is quite limited and not sufficient to
inhibitor (anastrazole) is currently under
allow making decisions likely to modify
investigation and the recruitment phase of
their own risk profile. The majority of
the study (IBIS 2) is closed.
women questioned do not appraise
correctly the risk factors they could act on
WOMEN'S VIEWS AND EXPECTA-
like alcohol consumption, physical activity
or weight control. Moreover two third
imply stress as one of the most important
A modern and efficacious approach
risk factor when no study has ever shown
of BC primary prevention supposes active
any direct causal link with BC. Adequacy
participation of women. Their behavior
of knowledge could well be linked to age.
depends on their understanding of the risk
However appropriateness of understanding
they run. Indeed the way they perceived
differs quite widely depending on the risk
the risk and their understanding of the
factor considered. For instance women
danger of dying from cancer seems far
aged between 40-59 years are better aware
from reality. Numerous studies conducted
of the importance exercise than women
in Europe and the US have revealed that
less than 40 or more than 60. Not
about 9 out of 10 women do not evaluate
surprisingly women with a family history
correctly their risk of developing BC. The
are better informed of risk factors on which
majority have very limited knowledge
they could act. The higher the education
concerning the risk factors they are
level, the higher the overall knowledge.
eventually exposed to (16). As of today we
Curiously patients referred by a GP do not
do not have data concerning the knowledge
score better for any question whatever the
and attitudes of the Belgian female
risk factor considered. More worrying 85%
population concerning primary prevention
of women participating in the survey had
of BC. However such information is
no idea at all of risk factors linked to BC.
paramount before deciding prevention
Concerning their willingness to take
strategies since some modifiable factors
medications or undergo surgery in high
risk situations, these women would simply
rely on the advice of their GP. One has to
replacement therapy or poor weight
know that as of today the medical
control). Moreover specific drug therapies
education does not offer any targeted
could be offered to high risk women. A
information on how the risk of BC should
recent survey was conducted in 1000
be screened and managed in high risk
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
populations. Most women would be
will benefit from any primary preventive
interested to participate in research
approach or might not be willing to follow
programs aimed at identifying new
it. However doctors have nowadays
preventive agents if they would be offered
effective tools in hands. The earlier the
any potential personal benefit. On the other
intervention in the causal cascade the
hand half of them (47%) would participate
longer the effects in reducing the risk and
anyway if the benefit would serve other
eventually decreasing the occurrence of
women. Unfortunately a single clinical
BC. In parallel huge efforts are needed to
trial in the field of primary prevention is
inform women on the modifiable risk
currently running in Belgium. On top this
factors, to educate the medical profession
study is limited to menopausal women. In
in evaluating individual risk, to foster
contrast several dozens of clinical trials
clinical research in the field of primary
sponsored by industry are being conducted
prevention. Public health efforts are also
but only aim at establishing new costly
required to develop consistent preventive
therapies to treat, not to prevent BC. Our
actions in parallel to mass screening.
survey confirms the lack of knowledge
within a high income Belgian population
In 2012 breast cancer is the leading
concerning their risk of developing BC. In
cause of female mortality due to cancer
this context it seems unlikely that these
and one of the most feared diagnoses by
women can make adequate choices and
women in this country. Today we master
take appropriate decisions in order to
better knowledge and have in hands
improve their risk profile.
effective tools to reduce a risk endangering
half of the population. Expectation would
CONCLUSION
suffer no excuse. What are we waiting for?
In order to fight effectively BC, the
role of prevention needs first to be recognized and acknowledged. Prevention seems a better alternative than therapy of overt disease. Nowadays major progress has been made and allows identifying more accurately those women at highest risk who could benefit most from preventive interventions. It is of crucial importance to establish the level of risk modifiable by surgery, drug therapy, behavioral changes and possibly tailored screening. Primary prevention strategies should be evaluated on an individual basis taking into account the general health state. Not all women
P Belg Roy Acad Med Vol. 2:.100-109
F. Liebens et al.
LIST OF REFERENCES
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers
12. Boyd NF, Martin LJ, Yaffe MJ, Minkin S.
C, Parkin DM. Estimates of worldwide burden
Mammographic density and breast cancer risk:
of cancer in 2008: GLOBOCAN 2008. Int J
current understanding and future prospects.
Cancer. 2010 ; 127:2893-917.
Breast Cancer Res 2011;13:223.
2. Belgian Cancer Registry. Fondation Registre du
13. Boyd NF. Tamoxifen, mammographic density,
Cancer. Statistiques du cancer en Belgique :
and breast cancer prevention. J Natl Cancer Inst
3. Parkin DM, Bray F, Ferlay J, Pisani P. Global
14. Rudel RA, Fenton SE, Ackerman JM, Euling
cancer statistics, 2002. CA Cancer J Clin. 2005;
SY, Makris SL. Environmental exposures and
mammary gland development: state of the
4. Recommandation pour le dépistage du cancer
science, public health implications, and research
dans l'Union Européenne Préparé par le groupe
recommendations. Environ Health Perspect.
des experts pour la prévention des cancers de
2011;119:1053–1061.
15. Cuzick J, Decensi A, Arun B, Brown PH,
Castiglione M, Dunn B., Forbes JF, Glaus A,
Howell A, von Minckwitz G, Vogel V,
5. Newman LA, Vogel VG. Breast cancer risk
Zwierzina H. Preventive therapy for breast
assessment and risk reduction. Surg Clin North
cancer: a consensus statement. Lancet Oncol.
Am. 2007;87:307-16.
2011;12:496-503.
6. Brown TA, Wall JW, Christensen ED, Smith
16. Mcmenamina M, Barry H, Lennon AM, Purcell
DV, Holt CA, Carter PL, Patience TH, Babu
H, Baum M, Keegan D, Mcdermot E,
SS, Williard WC. Atypical hyperplasia in the
O‟donoghue D, Daly L, Mulcahy H. A survey
era of stereotactic core needle biopsy. Journal of
of breast cancer awareness and knowledge in a
Surgical Oncology. 1998;67:168–173.
Western population: lots of light but little
7. Mahoney MC, Bevers T, Linos E, Willett WC.
illumination. European Journal of Cancer.
Opportunities and Strategies for Breast Cancer
2005;41: 393-397.
Prevention Through Risk Reduction. CA Cancer J Clin. 2008;58:347–371.
8. IARC working group on the evaluation of
cancer-preventive agents. Weight Control and Physical Activity. IARC Handbooks of Cancer Prevention, Volume 6. Lyon, France: IARC, 2002.
9. Mccormack VA, Boffetta P. Today's lifestyles,
tomorrow's cancers: trends in lifestyle risk factors for cancer in low- and middle-income countries. Ann Oncol. 2011;22: 2349-57.
10. McTiernan A. Behavioral Risk Factors in Breast
Oncologist. 2003;8: 326–334.
11. Danaei G, Vander hoorn S, Lopez AD, Murray
CJ, Ezzati M. Causes of cancer in the world: comparative risk assessment of nine behavioural and
2005;366:1784-93.
Source: http://probram.be/index.php/probram/article/viewFile/34/37
Jae-Min Jung and Ho-Yeon Kim: Third-person Effects in the Stock Market:Perception of Experts & Non-experts and Impacts on Attitude Third-person Effects in the Stock Market: Perception of Experts & Non-experts and Impacts on Attitude Jae-Min Jung* and Ho-Yeon Kim** Abstract: The third-person effect was tested by examining whether people perceive a greater influence of unidentified information recommending stocks in the Internet on others than on themselves. Findings confirm the third-person effect but also show subjects with stock market experience perceive a greater influence on others than did subjects with no stock market experience. Additionally, subjects demonstrated a larger third-person effect when "others" are specified as novice investors who have little knowledge or experience in stock trading than when "others" are identified as experienced traders. After controlling for SES and interest and experience in stock trading, the third-person perception remained. Keywords: Third-person perception, Behavioral effect, Stock market, Internet information, Expert
Duration of urination does not change with body sizePatricia J. Yanga, Jonathan Phama, Jerome Chooa, and David L. Hua,b,1 Schools of aMechanical Engineering and bBiology, Georgia Institute of Technology, Atlanta, GA 30332 Edited by David A. Weitz, Harvard University, Cambridge, MA, and approved May 14, 2014 (received for review February 6, 2014) Many urological studies rely on models of animals, such as rats and