Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Pone.0110358 1.14

Modeling the Dynamics of Disease States in Depression
Selver Demic1,2,3, Sen Cheng1,2,3*
1 International Graduate School of Neuroscience, Bochum, Germany, 2 Mercator Research Group ‘‘Structure of Memory'', Bochum, Germany, 3 Faculty of Psychology, Ruhr
University Bochum, Bochum, Germany
Major depressive disorder (MDD) is a common and costly disorder associated with considerable morbidity, disability, andrisk for suicide. The disorder is clinically and etiologically heterogeneous. Despite intense research efforts, the response ratesof antidepressant treatments are relatively low and the etiology and progression of MDD remain poorly understood. Herewe use computational modeling to advance our understanding of MDD. First, we propose a systematic and comprehensivedefinition of disease states, which is based on a type of mathematical model called a finite-state machine. Second, wepropose a dynamical systems model for the progression, or dynamics, of MDD. The model is abstract and combines severalmajor factors (mechanisms) that influence the dynamics of MDD. We study under what conditions the model can accountfor the occurrence and recurrence of depressive episodes and how we can model the effects of antidepressant treatmentsand cognitive behavioral therapy within the same dynamical systems model through changing a small subset ofparameters. Our computational modeling suggests several predictions about MDD. Patients who suffer from depression canbe divided into two sub-populations: a high-risk sub-population that has a high risk of developing chronic depression and alow-risk sub-population, in which patients develop depression stochastically with low probability. The success ofantidepressant treatment is stochastic, leading to widely different times-to-remission in otherwise identical patients. Whilethe specific details of our model might be subjected to criticism and revisions, our approach shows the potential power ofcomputationally modeling depression and the need for different type of quantitative data for understanding depression.
Citation: Demic S, Cheng S (2014) Modeling the Dynamics of Disease States in Depression. PLoS ONE 9(10): e110358. doi:10.1371/journal.pone.0110358
Editor: H. Sunny Sun, National Cheng Kung University Medical College, Taiwan
Received June 26, 2014; Accepted September 19, 2014; Published October 17, 2014
Copyright: ß 2014 Demic, Cheng. This is an open-access article distributed under the terms of the which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The authors confirm that all data underlying the findings are fully available without restriction. The code is freely available online at
Funding: S.C. was supported by a grant from the Stiftung Mercator. S.D. was supported by the International Graduate School of Neuroscience. The funders hadno role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* Email: [email protected]
for the involvement of specific genes and gene-by-environmentinteractions in the pathogenesis of MDD, even though they cannot
Major depressive disorder (MDD) affects around 20% of the
account for all occurrences of MDD [5].
population at some point during the life time of an individual [1–
One major theory about the biological etiology of depression
4]. Depression is a common and costly disorder that is usually
suggests that the underlying pathophysiological basis of depression
associated with severe and persistent symptoms leading to
is a depletion of the neurotransmitters serotonin, nor-epinephrine
important social role impairment, increased medical co-morbidity
or dopamine in the central nervous system [21–23]. Although
and mortality [5–7]. Depression can strike anyone regardless of
most antidepressants drugs (ADs) produce a rapid increase in
age, ethnic background, socioeconomic status or gender [8,9].
extracellular level of the monoamines, the onset of an appreciable
According to the World Health Organization, MDD is currently
clinical effect usually takes at least 3–4 weeks [24–29]. This
the leading cause of disease burden in North America and the 4th
delayed onset of action, or response, which is usually defined as a
leading cause worldwide [5,10–12]. The onset of MDD is usually
50% reduction in depression rating scale score compared to
between the ages of 20 and 30 years and peaks between 30 and 40
baseline [30], suggests that dysfunctions of monoaminergic
years [13,14].
neurotransmitter systems found in MDD represent the down-
The understanding of the nature and causes of depression has
stream effects of other, more primary abnormalities. In addition,
evolved over the centuries, though this understanding is incom-
success of AD treatment is relatively low. Selective serotonin re-
plete and has left many aspects of depression as a subject of
uptake inhibitors (SSRIs) are frequently used as a first medication
discussion and research. The heterogeneity of depression implies
for MDD, but have response rates of 50% to 60% in daily practice
that multiple neural substrates and mechanisms contribute to its
[31–35]. In some studies, ADs even fail to show superiority over
etiology [15]. Proposed causes include psychological, psychosocial,
placebo [36–38]. More precisely, the response to inert placebos is
hereditary, evolutionary and biological factors. Family, twin, and
approximately 75% of the response to active AD medication
adoption studies provide evidence that genetic factors might
[36,39]. The high rate of inadequate treatment of the disorder
account for some risk of developing MDD [16–18]. According to
remains a serious concern. Research comparing AD medication to
diathesis-stress theories of depression, genetic liability (diathesis)
cognitive behavioral therapy (CBT) has found that both are
interacts with negative life experiences (stress) to cause depressive
equally effective for non-psychotic forms of depression [40].
symptoms and disorders [19,20]. Indeed, there is some evidence
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
Indeed, in some theories of depression, cognitive aspects are
The variable M changes across time to account for changes in
dominant factors in the etiology and maintenance of the disorder
the symptoms and progression of MDD. We model the time
[41–43]. These models postulate that depressed patients process
evolution of M in discrete time steps according to this simple
depression-congruent information selectively, which seems to form
part of a vulnerability factor.
In addition to the heterogeneous etiology of MDD, the disorder
shows complex transitions between several disease states. Accord-
ing to the Diagnostic and Statistical Manual of Mental Disorder,
MðtzDtÞ MðtÞz
4th edition, text revision (DSM-IV-TR), the standard for thediagnosis of mental disorders, a depressive episode (DE) is
characterized as a period lasting at least 14 days, during which
In each time step Dt, the mood changes by the amount dM Dt.
the patient is consistently within the symptomatic range of a
The crucial issue is how to model the dynamics of the mood given
sufficient number of symptoms [1,44]. A DE can be interrupted by
by dM. The dynamics fully determines the behavior of the system
remission, which is defined as an asymptomatic period of at least
and should account for the major empirical observations in MDD
14 days [45]. A remission and recovery are accompanied by the
as outlined in the Introduction. We were looking for a simple
same behavioral symptoms and, at the behavioral level, distin-
model that can capture many of the important clinical observa-
guished only by their duration. A remission that lasts for 6 months
tions related to MDD. The simplest model is a linear one with a
or longer is called recovery [45]. This term refers to recovery from
single stable point. Preliminary work showed that linear dynamics
the episode, not from MDD per se. The appearance of a new DE
does not account for many important observations. It was too easy
after recovery is called a recurrence [45]. A relapse is a return of
to switch from positive to negative mood and vice versa, which is
the symptoms satisfying the full syndrome criteria for an DE
in contradiction with the phenomenology of MDD. Thus it was
during the period of remission, but before recovery [1,45].
evident that we needed a model that has two stable states, one
According to a population-based study among depressive patients,
corresponding to a depressive state and the other to a non-
about 15% of first lifetime onsets have unremitting course, and
depressive state. We therefore chose to model the dynamics with a
35% recover but have one or more future episodes [46,47]. These
polynomial of third degree (Fig. 1A).
cases may represent chronic and more severe forms of MDD[46,48]. About 50% of first lifetime onsets recover and have nofuture episodes [46]. However, the disease states in depression arenot defined consistently by different investigators, thus making it
dM {0:01aðM{bÞðM{cÞ M{
difficult to interpret the results and precluding comparisons
between different studies.
,where a.0; b, c, d are parameters to be studied, I is an external
All hypotheses that try to explain the dynamics of depression
input, and e is a Gaussian noise term with zero mean and a
have certain limitations, so our understanding what causes
standard deviation of one to set the scale. In our model, the system
depression is still incomplete. Existing hypotheses are not
is driven both by deterministic intrinsic dynamics (cf. Fig. 1B) and
exclusive, but rather complementary. The question is how to
a stochastic noise process (cf. Fig. 1C, D). The intrinsic dynamics is
integrate the different hypotheses. Mathematical models are well-
an abstract model of the changes in the mood of a person driven
suited for this problem. Here, we aim to systematically define the
by deterministic physiological processes, processes which we do
states in the course of MDD and to study the dynamics of MDD.
not attempt to model mechanistically here. The dynamical system
We developed a single abstract model that is consistent with many
in Eq. (2) has two stable fix points, separated by an unstable fix
existing theories about depression. Although our model is not
point. The parameters b, c, and d are ordered such that bƒcƒd
mechanistic, it helps us to understand and analyze the etiology and
(Fig. 1A). The parameters of the model specify the unique
dynamics of MDD. Finally, we modeled the influence of three
dynamics of a system, which represents a person. Depending on
types of therapies (antidepressant treatment, cognitive behavioral
how the parameters affect the dynamics of MDD, we assign them
therapy, and life style changes) on the occurrence and duration of
to possible physiological correlates (Table 2). Within a subpopu-
depressive episode.
lation in our model, all individuals share identical parameters. Bycontrast, the noise process captures stochastic physiological
processes as well as external environmental factors. Fluctuations
Dynamical systems model of major depressive disorder
in the mood can be caused, for instance, by random hormonal
To model the dynamics of depression, we first need a way to
changes or by changes due to the circadian rhythm. Also, external
describe the state of a person, i.e., whether a person is suffering
changes might cause fluctuation in the mood of a person during
from MDD or not. We adopted the simplest approach possible,
the day, i.e., stressful situations at work or rapid weather changes.
which is to describe the state of a person by a single variable. We
The name ‘‘noise'' does not imply that the noise process is
call this variable M, loosely for mood. M,0 indicates that the
irrelevant or unimportant. On the contrary, the noise term is
person suffers from symptoms associated with MDD; the person is
crucial in our model since it introduces unpredictable changes to
in the symptomatic state. In our simple model with only one
the mood. This stochasticity is what makes the time-course of the
variable, we do not model which precise symptoms patients suffer
mood of one modeled person (cf. Fig. 1D) different from that of
from. A negative value of the state variable indicates that the
another person.
person satisfies a sufficient number of symptoms (Table 1) to meetthe syndromal criterion for a depressive episode according to
Relating occurrence and recurrence rates to the
DSM-IV-TR [1]. If this state persists for fourteen days or more,
distribution of the number of depressive episodes
the person is considered to suffer from MDD [1,45]. M.0
We use empirical occurrence and recurrence rates to compute
indicates that the person does not meet the syndromal criterion for
the distribution of the number of depressive episodes during an
a depressive episode; the person is in the asymptomatic state.
individual's lifetime (NDE) since the latter is rarely reported by
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
Table 1. DSM-IV-TR Criteria for Major Depressive Disorder [1].
Five or more of the following symptoms should be present daily formost of the day for at least 2 weeks
The rate of first recurrence RRð1Þ is the fraction of patients
At least one symptom is either depressed mood or anhedonia
who suffer from depression a second time out of those patients whosuffered from one previous depressive episode. The rates of second
Changes in appetite or weight
recurrence RRð2Þ, third recurrence RRð3Þ, etc. are defined
Insomnia or hypersomnia
similarly. In general, RRðiÞ can be calculated using the following
Psychomotor agitation or retardation
Fatigue or loss of energy
Feelings of guilty or worthlessness
Difficulty with thinking, concentrating, or making decisions
Suicidal ideation or suicidal attempts
The probability of having no depressive episode is
epidemiological studies but quite informative. The occurrence rate(OR) is the fraction of the population that suffers from at least one
DE during their life time. The OR thus equals the probability ofhaving one or more depressive episodes, i.e.,
The probability of having exactly one depressive episode is
Figure 1. Dynamical systems model for the dynamics of mood. A) A schematic showing the mood change as a function of the state variableM without external inputs and noise (I = e = 0). The arrows at 1, 2, 3, 4 indicate the direction of change in those states. The points labeled with b, c, andd are fix points. At these points, the value of the change is zero (dM/dt = 0). Therefore, when there is no noise, the state will not change once it hasreached a fix point. The fix points b and d are stable, meaning that the system will return to these states if slightly perturbed. The fix point c isunstable and has different properties, the system will move further away from point c even if the system is only slightly perturbed. In that case, thesystem will evolve until it reaches one of the stable fixed points. If Mwc, the system will move towards the fix point d. The system will evolve towardsthe other fix point b, if Mvc. Therefore, the fix point c separates the basins of attraction of the two stable fix points. Samples of the evolution of Mover time B) without noise, C) with a moderate level of noise and D) with high level of noise. Note, that with high level of noise the system exhibitsstochastic transition between positive and negative values.
doi:10.1371/journal.pone.0110358.g001
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
Table 2. Potential physiological correlates of the model parameters.
Potential physiological correlates
Hippocampal volume and rate of adult neurogenesis
Negative stable fix point
Level of monoamines (i.e. serotonin)
Instable fix point
Pessimistic attitude c.0, optimistic attitude c,0
Positive stable fix point
Amygdala activity (higher activity is represented by a smaller d)
Environmental influence
Unpredictable internal or external changes that cause fluctuation in the mood
Finite state machine: systematic definition of disease
1� ð1{RRð1ÞÞOR
We developed a finite state machine (Fig. 2) to systematically
The probability of having two or more depressive episode is
define the disease states of MDD: depressive episode, remission,
computed according to this equation
recovery, and relapse, which were described above. This mathe-matical model analyzes the transitions of M from the asymptom-atic to the symptomatic state, and vice versa, and assigns a disease
p½NDE i� ð1{RRðiÞÞOR P RRð jÞ
state to each time interval. The disease state changes depending on
the length of periods for which M remains positive (Tp) or negative(Tn) (see Fig. 3 for an example). In addition to the disease states of
clinical relevance, we had to introduce auxiliary disease states to
To study the OR and RR, we initialized the system in a positive
account for short interruptions of a disease state that are clinically
state Mð0Þ 1:75 and simulated the dynamics of MDD for a
irrelevant. For instance, if a one-month-long depressive episode is
period of 70 years using a time-step Dt 0:1d. For both the single
interrupted by a 2-day-long period in the asymptomatic state,
population and the two sub-populations model, the analyses are
there is little reason to assume that the short interruption has any
based on simulations of 10000 individuals. In the two sub-
relevance. Clinicians frequently make such intuitive judgments
populations model, 93% of individuals belong to the low-risk sub-
without making them explicit [45], but such discounting has to be
population while the remaining 7% belong to the high-risk sub-
build in explicitly in a mathematical model.
In the following, we describe the auxiliary disease states in more
detail. The null state is the initial state, before any data is available
Studying treatment effects
to make a more specific determination of the disease state. Short
To study the time-to-remission and time-to-response in our
periods in the symptomatic state, Tnv14, and any duration in the
model, we initialized the system in a negative state bƒMð0Þv0.
asymptomatic state, Tpw0, will not change this state (Fig. 2&3).
The initial value was drawn from a uniform distribution. We
The only possible transition out of the null state is to a DE, if the
simulated the dynamics of MDD for a period of 20 years using a
syndromal criterion is met for at least 14 consecutive days, i.e.,
time-step Dt 0:1d. To study the effects of different treatments, we
Tn§14. A rebound depressive episode is an interruption of a DE
used only simulations of the two-subpopulations model in which a
that is shorter than two weeks (Fig. 2&3). The duration in the
DE occurred. Hence, 63% of the simulations belong to the low-
positive state is added to the duration of the DE (boxes connected
risk sub-population while the remaining 37% belong to the high-
to rebound depressive episode in Fig. 2). Similarly, rebound
risk sub-population. We initialized the finite-state machine in the
relapse, interrupted remission, and interrupted recovery are
rebound depressive episode state and considered the time when M
interruptions of the relapse, remission and recovery states of
increases above 50% as time-to-response, and the time at which
MDD, respectively. The auxiliary disease states are necessary to
the first remission or recovery occurred as the time-to-remission.
discount short interruptions of the disease states in our model and
Fourteen days were added to the time-to-remission to account for
have little clinical relevance. We therefore focus our attention on
the fact that symptoms have to be present for at least fourteen days
the clinically relevant disease states in the following.
to qualify as an DE. In the control group, parameters were
One point requires special attention. Recovery occurs after an
identical to those used for the simulation of the occurrence rate. In
asymptomatic period of 6 months or more, even if that period is
the experimental group, we changed certain parameters in order
interrupted by short periods (,14 days) in the negative state. If the
to simulate the effect of various treatments such as AD treatment
first period in the positive state lasts for longer than 14 days and
(change in parameter a, and d or b), CBT (change in parameter c)
less than 6 month, then the finite-state machine will initially label
and life style changes (change in parameter I).
this period as remission. Short interruptions in the negative state
All simulations and analyses were performed in Matlab R2012a
and the following periods in the positive state are added to
(MathWorks; Natick, Massachusetts, USA) using custom-written
duration of remission. If the total duration of the ‘‘remission''
software. The code is freely available online at
period exceeds 6 months, then the period becomes recovery. To
correct the initial classification, we included an action ‘‘change
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
Figure 2. Finite state machine modeling the transitions between the disease states in depression. State diagram for the finite statemachine. Ellipses represent the disease states in depression. Grey filled ellipses are clinically relevant disease states; unfilled ellipses are auxiliarydisease states that are needed to discount short interruptions of clinically relevant disease states. The arrows indicate transitions between diseasestates. Transitions only occur when the state variable M changes sign, i.e., either from positive to negative, or vice versa. Each arrow is labeled by thecriteria that trigger the transition. Tn represents the length (in days) of the period during M,0 before transition to a positive value occurred. In otherwords, Tn is the duration that a person meets the syndromal criterion for a depressive episode according to DSM-IV-TR [1]. Accordingly, Tp representsthe length (in days) of the period during M.0, i.e., the duration in which a person does not meet the syndromal criterion for a depressive episode.
The rectangles indicate a change to previously identified states. Short interruptions of disease states are added to the duration of disease states.
doi:10.1371/journal.pone.0110358.g002
previous state'' (Fig. 2). This finite-state machine unambiguously
Dynamical systems model for the dynamics of major
defines the disease states and can be used to track their evolution
depressive disorder
over the lifespan of patients as well as in our theoretical
We developed a simple dynamical systems model (see Methods)
to simulate and study the progression of disease states over 70
Figure 3. Example of the time course of the state variable M and the disease states identified by the finite state machine. In thisexample, a symptomatic period lasting 28d is interrupted by an asymptomatic period of 5d and followed by another symptomatic period of 27d.
Therefire, our model identifies the three periods together as a single depressive episode of length 60d. Tn and Tp represent the length (in days) of theperiod when M,0 and M.0, respectively.
doi:10.1371/journal.pone.0110358.g003
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
years. In a first attempt, we speculated that perhaps all people
that treatment with AD increases the rate of adult neurogenesis in
share the same dynamics parameters, and thus similar physiolog-
the dentate gyrus [49] and it has been suggested that adult
ical parameters, and that depressive episodes occur stochastically.
neurogenesis is important for memory [50]. Since the parameter a
If our model captures some aspect of the dynamics of MDD, it
determines how quickly the current state is forgotten, we
should be able to account for the epidemiological data on
hypothesized that AD treatment increases parameter a. Since
occurrence and recurrence rates of MDD (see Methods).
the intended effect of AD treatment is to reduce the time that
patients suffer from the symptoms of MDD, we decided to use the
RR(2) = 70%, and RR(3) = 90% [1]. In our first modeling
time-to-remission as the target parameter for AD treatment. Our
attempt, we chose a single set of parameters representing a
simulation results contradict our initial hypothesis, increasing the
homogeneous population to match the epidemiological occurrence
parameters a and d increases, rather than decreases, the time-to-
rate. The parameters of the single population model were:
remission (Fig. 7B&C). One potential resolution could be to
a = 4.65; b = 23; c = 0.175; d = 5; I = 0.02. However, this
assume that we correctly guessed the physiological correlates of the
model does not match any of the epidemiological recurrence rates
parameters a and d, but the relationship is inverse to our
(Fig. 4A). The mismatch is not simply a numerical issue, the model
expectation. However, this interpretation is inconsistent with the
yields qualitatively different data. Rather than having rates that
OR in our simulations. Decreasing parameters a and/or d,
increase with the number of DE as in epidemiological studies, in
increases the OR. Thus if we modeled the effect of AD treatment
our single-population model, the rates decrease.
as a decrease in parameters a and/or d, it would imply
This is not surprising. Since a one-dimensional model has no
paradoxically that AD treatment of healthy patients increases
memory other than the current state, the probability of the second
the OR of MDD (Fig. 7A, C). An extensive parameter search did
DE (the first recurrence) occurring within a certain time period is
not yield any parameter changes in a and d that have the desired
the same as the probability of the first DE. However, the first DE
change time-to-remission and OR simultaneously. We therefore
can occur anytime within the full 70 years of simulated time
turned to model the increase in the level of monoamines as an
whereas the second DE can only occur after the first DE had
increase in parameter b (Fig. 8). In this scenario, the time-to-
already occurred. Since the number of DE are proportional to the
remission is reduced by an increase in b, but elevated by an
length of the observation period, the first recurrence rate is lower
increase in a (Fig. 8B, E). While the latter outcome is an
than the occurrence rate. The same logic applies to the second and
undesirable property, there are combinations of simultaneous
third recurrence rates, which are successively lower (Fig. 4A). Our
increases in parameters a and b that yield a lower time-to-
argument implies that this property is not specific to the particular
remission. This is possible because the contour lines are not
parameters that we chose. Indeed, additional simulations show for
parallel to the axes or, in other words, the parameters are inter-
a range of the parameters a and b that, in the single population
dependent. Similarly, the OR is reduced by an increase in a, as
model, the rate of first recurrence is lower than the occurrence
desired, but elevated by an increase in b (Fig. 8A, C). Again, there
rate, and the rate of second recurrence is lower than the rate of
are combinations of simultaneous increases in parameters a and b
first recurrence (Fig. 5). To further investigate how the single
that yield a lower occurrence rate. Importantly for the change of
population model deviates from the true dynamics of MDD, we
parameters indicated by the black and white points, representing
calculated the distribution of NDE (Fig. 4B). In the simulated data,
pre- and post-treatment parameters, the change in both the time-
the likelihood monotonically decreases such that four or more DE
to-remission and occurrence rate are in the desired directions. We
are absent from our simulated data. In contrast, the epidemiolog-
therefore suggest that parameter a correlates with the rate of adult
ical data show that four or more DE occur with a substantial
neurogenesis and parameter b with monoamine levels (Table 2). It
probability of around 7% and is even higher than the probability
is worthwhile to note that AD treatment in our model does not
of two or three DE. Since the epidemiological data follows a
work like a deterministic switch. Even though AD treatment in our
bimodal distribution, we hypothesized that two subpopulations
model alters the physiological parameters immediately, remission
might be required to account for empirical occurrence and
remains a stochastic process driven by the intrinsic dynamics and
recurrence rates of MDD.
the noise term. The results of our model demonstrate that the time
We therefore simulated data for two sub-populations. In this
required to see a significant effect of antidepressants is about three
model, ninety-three percent of the population shares low-risk
weeks, which is highly similar to the epidemiological data (see
parameters and develops depression with low probability. The
Table 3). Figure 9 shows the distribution of the duration of DEs.
parameters of this sub-population were chosen (a = 5; b = 22.85;
Both the treated (Fig, 9D, E, F) and control groups (Fig. 9A, B, C)
c = 0.175; d = 5; I = 0.02) such that OR = 13%. The remaining
exhibit distributions with large variances and long tails. This result
seven percent of the population belongs to the high-risk sub-
is somewhat surprising given that within each subpopulation all
population and develops depression with very high probability
individuals share the same parameters and it underlines the
(,100%). The parameters for this sub-population were: a = 4.4;
difficulty in understanding the physiological mechanisms of AD
b = 23.75; c = 0.175; d = 4.25; I = 0. At this point, we would
treatment. These highly skewed distributions might explain why
like to stress that the two sub-populations together represent the
the median duration of depressive episodes reported in the
entire population, which implies that no one is absolutely immune
literature varies widely from three to twelve months, even if most
to depression. By design, the two sub-population model yields a
studies suggest that the median duration of depressive episode is
bimodal distribution of NDE (Fig. 6B). With this two sub-
about three months [51–56]. Overall, we find that our model
population model, we were able to match the empirical occurrence
reproduces rather well other variables which are often used in a
and recurrence rates of MDD (Fig. 6A).
clinical and epidemiological studies to examine the efficacy of ADtreatment (Table 3).
Modeling the effect of antidepressant treatment
The most commonly used antidepressants are those that
Modeling the effects of cognitive behavioral therapy and
regulate the metabolism of monoamines in the brain, in particular
life style changes
serotonin. Our initial hypothesis was that the parameter d
CBT instructs patients with MDD to develop a more optimistic
correlates with monoamine levels. Furthermore, it was shown
approach to life and to detect and transform negative thoughts
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
Figure 4. Single population model can account for empirical occurrence rate but not for recurrence rates. A) The occurrence rate (OR)from our simulation (grey bars) was fit to the result from epidemiological studies (black bars). The parameters of the model are: a = 4.65; b = 23;c = 0.175; d = 5; I = 0.02. However, in our simulation, the recurrence rates, RR(i), decrease with the number of prior depressive episodes, which iscontrary to epidemiological data. B) The distribution of the number of depressive episodes (DE). The probability of zero DE is 0.8. The bars were cutoff to show more clearly the smaller probabilities for the higher numbers of DE. The epidemiological distribution is clearly bimodal (black bars),whereas the simulated distribution is unimodal (grey bars).
doi:10.1371/journal.pone.0110358.g004
into positive thinking [40,57,58]. The effect of CBT is an
Life style changes such as, for instance, exercise, social support,
improved ability to deal with difficult circumstances and shorter
and stress reduction lead to a lower probability of having another
durations of DEs [59,60]. A similar effect occurs in our simulations
DE and to shorter duration of DEs, if they do occur [61–63].
when we decrease parameter c: both the OR and the time-to-
Indeed, a recent study compared exercise, antidepressant medi-
remission decrease (Fig. 10, the black and white points represent
cation and combined medication and exercise in adults and found
pre- and post-treatment value of parameter c, respectively).
that all treatments were effective [61,62]. Since external factors
Moreover, the results of our model show that about half of the
enter our model through the parameter I, we suggest that the
patients treated with CBT will be in remission after three months
parameter I correlates with environmental influence, where larger
of treatment and that the number of patients in remission increases
I corresponds to positive environmental influence and smaller I to
with elapsed time, in line with the epidemiological data (see
negative influence (Table 2). Our simulations confirm that
Table 3). Hence, we hypothesize that smaller c correspond to
increasing I indeed decreases the time-to-remission and the OR
optimistic attitude and larger c to pessimistic attitude (Table 2).
(Fig. 10). In addition, our results suggest that the combination of
Figure 5. Influence of parameters a and b on the occurrence and recurrence rate in the single population model. A) Occurrence rate,B) first recurrence rate, and C) second recurrence rate, each represented by color scales, for a range of the parameters a and b. The remainingparameters are: c = 0.175; d = 5; I = 0.02. Note, that for all combinations of the parameters a and b, the rate of first recurrence is lower than theoccurrence rate, and the rate of second recurrence is lower than the rate of first recurrence.
doi:10.1371/journal.pone.0110358.g005
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
Figure 6. Two sub-population model can account for empirical occurrence and recurrence rate. A) The parameters of the two sub-population model are: a = 5; b = 22.85; c = 0.175; d = 5; I = 0.02 for the low-risk sub-population and a = 4.4; b = 23.75; c = 0.175; d = 4.25; I = 0 for thehigh-risk sub-population. Our simulation data (grey bars) closely matches the empirical (black bars) occurrence and recurrence rates and B) thedistribution of the number of depressive episodes.
doi:10.1371/journal.pone.0110358.g006
the two interventions, CBT and life style changes, will yield better
model, it incorporates several parameters that can be associated
results in the treatment of depression and the prevention of
with physiological mechanisms. The advantage of this model is
relapses and recurrence than their individual application.
that it can incorporate several biological and psychological factorsthat are thought to affect MDD, and describe their potential
interactions. Combining the finite-state machine and dynamicalsystems model, we studied the dynamics of disease states in
In this article, we have developed a finite-state machine to
depression and found that two sub-populations, one high-risk and
systematically define the states in the course of MDD together with
one low-risk, are required in our model to account for the
operational criteria for the terms remission, recovery, relapse, and
empirical data. The two sub-populations model is able to
recurrence. We used a simple dynamical systems model to
reproduce many, though not all, observations quite well.
simulate the day-to-day fluctuations in the mood that might
One parameter, d, we have not associated with a physiological
correlate with depression. While this model is not a physiological
or cognitive roles, yet. The influence that parameter d has on the
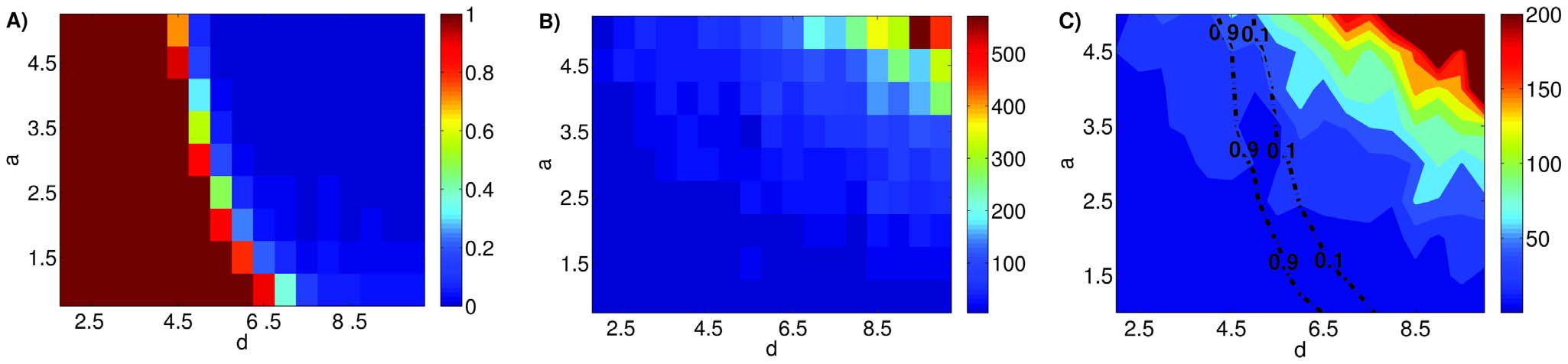
Figure 7. Modification of parameters a and d cannot account for the effect of antidepressant treatment. Shown in the color scales arethe occurrence rate (A), the median time-to-remission (B) and the contours of the median time-to-remission (C) in simulated data. Consistent withthe assumption that monoamine levels correlate with parameter d and the rate of adult neurogenesis with parameter a, the occurrence ratedecreases with increasing parameters a and d (A). However, modeling the effect of antidepressant treatment as increases in parameters a and dwould make the paradoxical prediction that antidepressant treatment increases the time-to-remission (B). C) To show this conflict more explicitly weplot both the occurrence rate and the time-to-remission in the same panel. The dashed lines represents contours in the occurrence rate at theindicated values, while the color scale represents median time-to-remission. It is highly unlikely to find parameter combinations of a and d whichreduces the time-to-remission while keeping the occurrence rate constant or lowering it.
doi:10.1371/journal.pone.0110358.g007
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
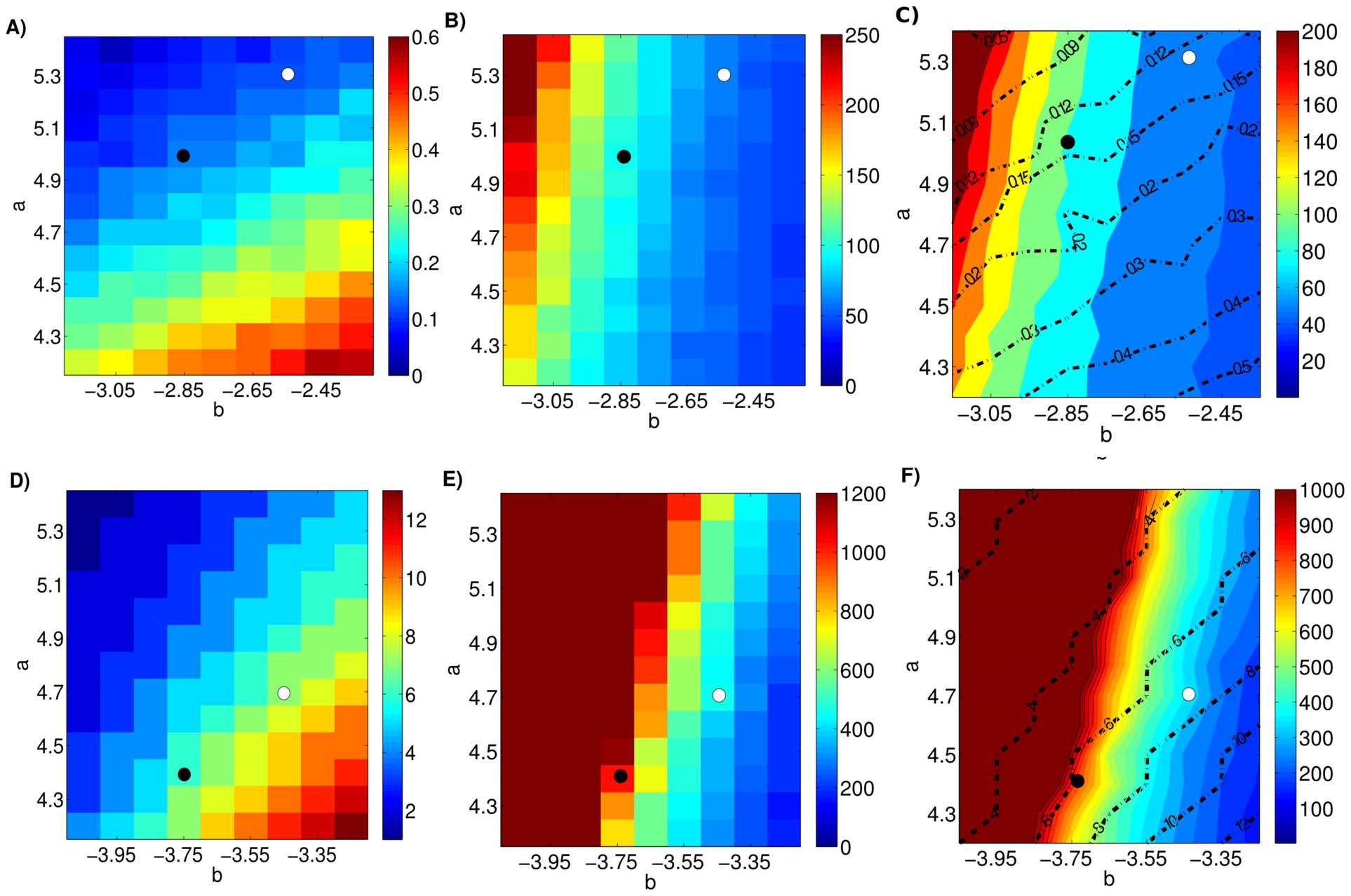
Figure 8. Increases in parameters a and b are consistent with the effect of antidepressant treatment. The first row of panels shows theresults of simulations for the low-risk sub-population where the color scales in A) and B) represent the occurrence rate and median time-to-remission,respectively. Panel C) displays the same data using contour lines (occurrence rate) and color scale (media time-to-remission). The second row ofpanels shows the results for the high-risk sub-population where the color scale represents D) the median number of depressive episodes and E)median time-to-remission. Panel F) displays the same data using contour lines (median number of depressive episodes) and color scheme (mediantime-to-remission). The black and white points mark pre- and post-treatment parameters, respectively. For certain parameter combinations anincrease in the parameters a and b reduces the median time-to-remission while keeping the occurrence rate (the median number of depressiveepisodes for the high risk sub-population) constant or lowering it.
doi:10.1371/journal.pone.0110358.g008
occurrence rate and time-to-remission suggests that d might
condition, and model the dynamics of MDD with a continuous
correlate partly with amygdala activity. Indeed, other authors
state variable (M). However, since virtually all existing observa-
before us have tied the amygdala to depression [64,65].
tions on MDD have been based on categorical classification and
Hyperactivity in the amygdala is a common finding during
clinical practice depends on it, we developed the finite-state model
baseline conditions in MDD [66] and has been interpreted as a
to translate between the dynamics of a continuous one-
valence-specific effect that causes a negative memory bias [67,68].
dimensional system and the categorical classification of diseasestates. Since we are at an early stage of the modeling process, it
Dimensionality of the model and history-dependence
appeared prudent to start with a single state variable to model the
DSM-IV-TR, used worldwide as a diagnostic tool, does not
dynamics of MDD, especially given the paucity of data that could
define absolute boundaries between mental disorder and no
constrain higher-order systems. In addition, the general approach
mental disorder. However, the use of a categorical classification is
in modeling is to start with a parsimonious model and to include
fundamental in everyday clinical practice and research, as well as
more complexity only if and when additional mechanisms are
for health services and insurance purposes. The categories are
required. So far, the simple model we studied has been able to
prototypes, which define certain criteria related to symptoms, i.e.,
account for a surprisingly wide range of observations.
we say that a patient with a close approximation of the ill-
A consequence of the choice of a one-dimensional model is that,
prototype is ill. However, it has been argued that MDD should not
at a given point in time, the system's behavior is fully determined
be treated as a categorical condition and instead be viewed along a
by the one state variable. As a result, the system does not depend
continuum [69]. Instead of categorizing subjects as ill or healthy,
on the previous history of the system. For instance, the probability
they should be scored on a graded scale according to how may
of developing a DE does not depend on whether the patient has
symptoms the subject expressed and/or how severe the symptoms
previously experienced a DE or not. To allow the history to affect
are. Some authors go even further to suggest that a one-
the behavior of the system, we would have to include additional
dimensional approach is not sufficient and that multiple dimen-
state variables which would imply more complex higher-order
sions have to be used to capture the multiple facets of depression.
systems. We are aware that to fully understand depression, it
In this study, we reject the view that depression is a categorical
eventually will be necessary to incorporate such history-depen-
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
Table 3. Comparison of quantitative measures of disease progression between model and clinical observation.
Occurrence rate, OR
1st recurrence, RR(1)
2nd recurrence, RR(2)
3rd recurrence, RR(3)
Mean time-to-response
2 to 3 we [26], 3 to 4 we [24], 20 to 31 we [87]
DE duration in patients treated with AD (from onset of DE to remission/recovery)
3 mo [51], 16 we [82], 22 we (1st DE) [55], 19 we
50% [51], 53% [60]
12% [84],15% [46], 20% [51], 20% [54], 22% [83]
DE duration in patients treated with AD (from onset of AD treatment toremission/recovery)
Median age of onset of 1st DE
early-to-mid twenties [84]
DE duration in patients treated with CBT
p(TDE, = 16 week)
AD: antidepressant; DE: depressive episode; TDE: duration of depressive episodedoi:10.1371/journal.pone.0110358.t003
dence. For instance, epidemiological studies have found evidence
3 months and a long tail including episodes longer than 9 years.
that adverse experience during childhood, such as sexual or
The properties of this distribution suggests two things. First, many
physical abuse, neglect or loss of parents, is associated with
studies were not able to see an effect of the AD treatment because
substantial increase in the risk of developing depression [70–73].
the time window of observation was not long enough. Second, any
Additionally, childhood trauma can change symptom patterns and
effect of AD treatment is highly variable. Note that the parameters
the clinical course of MDD. For example, childhood trauma has
are identical for each simulation, so the widely different durations
been consistently associated with an early onset of depression
of depressive episodes did not emerge as a result of differences in
[74,75], as well as larger numbers of depressive episodes or more
the parameters. Furthermore, the risk of relapse seemed similar
chronic depression [76,77]. Moreover, childhood adverse experi-
across heterogeneous groups of patients including those who had
ence has been associated with a decreased responsiveness to
recently responded to treatment of an acute episode and those who
pharmacological treatment in patients with dysthymia and
had been successfully taking maintenance treatment for several
depression [78,79]. However, not all forms of depression are
months or even years [80]. Similarly, our modeling results indicate
associated with childhood adversity, and we may speculate that the
that AD treatment does not decrease the probability of developing
high-risk sub-population in our model may partly include the
another DE in the future.
group of depressive patients with a history of childhood trauma.
Indeed, patients within the high-risk sub-population in our model
Practical implications
tend to have more episodes, longer duration of episodes as well as
Our results imply that people who suffer from depression can be
more chronic episodes than those in the low-risk sub-population.
assigned to two sub-populations. The low-risk sub-populationdevelops depression by chance, and those from this sub-population
Comparison between observations and model outputs
who suffer from MDD do not otherwise differ from those who
Our model offers an account for why AD treatment has only
never develop depression. The high-risk sub-population has an
low rates of success and in some studies did not show superiority
increased likelihood of developing depression, and tends to have
over placebo [36–38]. In our model, the distribution of DE
more DEs during their life time, and longer DE durations. This
durations in the treated patients is very broad with a peak at about
prediction of our model may have relevance for clinicians, because
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
Figure 9. Distribution of the duration of depressive episodes. A), B), and C) show data for control group with pre-treatmentparameters. D), E), and F) show data for treatment group with post-treatment parameters. The first row (A, D) of panels shows theduration of depressive episodes for the low-risk subpopulation, the second row (B, E) for the high-risk subpopulation, and the third row (C, F) for thejoint distribution. Note that the distributions have long tails, indicating that some patients take much longer to improve than others, even thoughthey all share the same parameters.
doi:10.1371/journal.pone.0110358.g009
it suggests that the patients who belong to the high-risk sub-
quantitative data for understanding depression. We therefore hope
population are at high risk of developing a chronic course of the
that our modeling work will promote new empirical studies and/or
disease. Moreover, this group of patients demands long-term
reexaminations of existing data. In particular, we believe that it is
treatment and regular check-ups after recovery.
important to monitor the disease progression in MDD on a day-to-
We do not claim that our model is the final word on modeling
day basis. The finite-state machine model that we developed here
the dynamics of depression. On the contrary, it has several
could be used to define the disease state of MDD more consistently
apparent limitations some of which we have discussed above. The
and the operational criteria we suggested here might lead to
main goal of our article is to show the potential power of
improved design, interpretation, and comparison of studies of the
computationally modeling depression and the need for different
natural course and clinical therapeutic trials. Ultimately, we hope
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
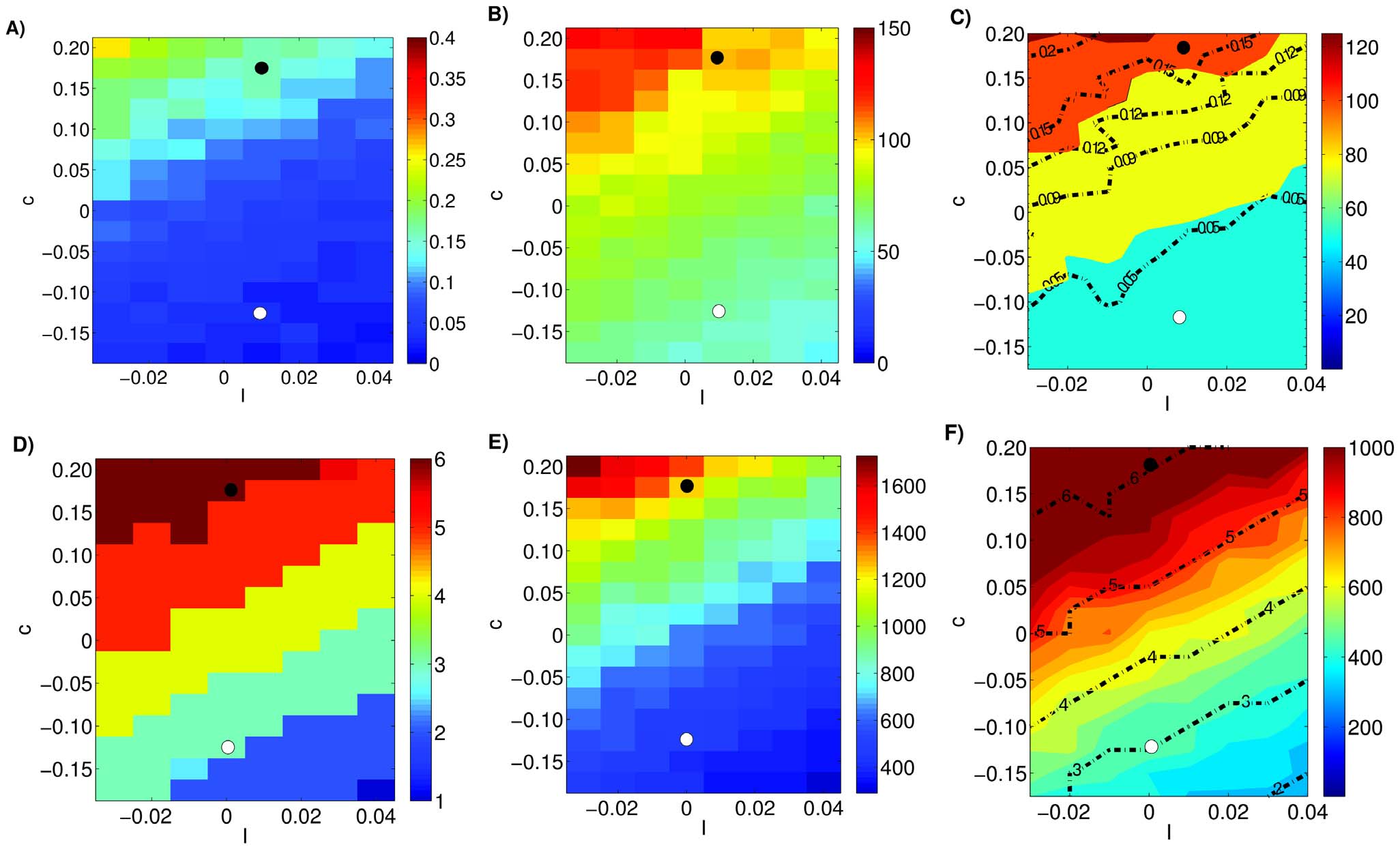
Figure 10. Modeling the effect of cognitive behavioral therapy and life style changes on MDD. Plotting convention as in Figure 8. Anincrease in the parameter I and/or decrease in c reduces the occurrence rate (A) (the median number of depressive episodes for the high-risk sub-population, D) and the median time-to-remission (B and E). These results suggests that smaller values of parameter c correlates with more positiveattitude and larger values of I correlate with more positive environmental influences.
doi:10.1371/journal.pone.0110358.g010
that such efforts will lead to a clearer understanding of the nature
Author Contributions
Conceived and designed the experiments: SD SC. Performed theexperiments: SD SC. Analyzed the data: SD SC. Contributed reagents/
materials/analysis tools: SD SC. Wrote the paper: SD SC.
We thank Martin Bru¨ne for helpful comments on an earlier version of themanuscript.
1. American Psychiatric Association (2000) Diagnostic and Statistical Manual of
9. Nolen-Hoeksema S (2001) Gender Differences in Depression. Current
Mental Disorders IV Edition Text Revision (DSM IV TR). Washington DC,
Directions in Psychological Science 10: 173–176. doi:10.1111/1467-8721.
2. Blazer DG, Kessler RC, McGonagle KA, Swartz MS (1994) The prevalence and
10. Kessler R, Berglund P, Demler O, Jin R, Koretz D, et al. (2003) The
distribution of major depression in a national community sample: the National
epidemiology of major depressive disorder: results from the National
Comorbidity Survey. The American journal of psychiatry 151: 979–986.
Comorbidity Survey Replication (NCS-R). JAMA: the journal of the American
3. Hasin DS, Goodwin RD, Stinson FS, Grant BF (2005) Epidemiology of major
Medical Association 289: 3095–3105. doi: doi: 10.1001/jama.289.23.3095.
depressive disorder: results from the National Epidemiologic Survey on
11. Greenberg PE, Kessler RC, Birnbaum HG, Leong SA, Lowe SW, et al. (2003)
Alcoholism and Related Conditions. Archives of general psychiatry 62: 1097–
The economic burden of depression in the United States: how did it change
between 1990 and 2000? The Journal of clinical psychiatry 64: 1465–1475.
4. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, et al. (2005)
12. Murray CJ, Lopez AD (1996) Evidence-based health policy—lessons from the
Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the
Global Burden of Disease Study. Science (New York, NY) 274: 740–743.
National Comorbidity Survey Replication. Archives of general psychiatry 62:
13. Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, et al. (1994)
Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the
5. Hasler G (2010) Pathophysiology of depression: do we have any solid evidence of
United States. Results from the National Comorbidity Survey. Archives ofgeneral psychiatry 51: 8–19. doi: 10.1001/archpsyc.1994.03950010008002.
interest to clinicians? World psychiatry: official journal of the World Psychiatric
14. Kessler RC, Bromet EJ (2013) The epidemiology of depression across cultures.
Association (WPA) 9: 155–161.
Annual review of public health 34: 119–138. doi:10.1146/annurev-publhealth-
6. Angst F, Stassen HH, Clayton PJ, Angst J (2002) Mortality of patients with mood
disorders: follow-up over 34–38 years. Journal of affective disorders 68: 167–181.
15. Nestler E, Barrot M, DiLeone R, Eisch A, Gold S, et al. (2002) Neurobiology of
7. Murray CJ, Lopez AD (1997) Global mortality, disability, and the contribution
depression. Neuron 34: 13–25.
of risk factors: Global Burden of Disease Study. Lancet 349: 1436–1442.
16. Sullivan PF, Neale MC, Kendler KS (2000) Genetic epidemiology of major
depression: review and meta-analysis. The American journal of psychiatry 157:
8. Weissman MM (1996) Cross-National Epidemiology of Major Depression and
Bipolar Disorder. JAMA: The Journal of the American Medical Association 276:
17. Flint J, Kendler KS (2014) The Genetics of Major Depression. Neuron 81: 484–
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
18. Kendler KS, Gatz M, Gardner CO, Pedersen NL (2006) A Swedish national
46. Eaton W, Shao H, Nestadt G, Lee HB, Lee BH, et al. (2008) Population-based
twin study of lifetime major depression. The American journal of psychiatry 163:
study of first onset and chronicity in major depressive disorder. Archives of
general psychiatry 65: 513–520. doi: 10.1001/archpsyc.65.5.513.
19. Monroe SM, Simons AD (1991) Diathesis-stress theories in the context of life
47. Hardeveld F, Spijker J, De Graaf R, Nolen WA, Beekman ATF (2010)
stress research: implications for the depressive disorders. Psychological bulletin
Prevalence and predictors of recurrence of major depressive disorder in the adult
110: 406–425.
population. Acta psychiatrica Scandinavica 122: 184–191. doi:10.1111/j.1600-
20. Hornung OP, Heim CM (2014) Gene-Environment Interactions and Interme-
diate Phenotypes: Early Trauma and Depression. Frontiers in endocrinology 5:
48. Torpey DC, Klein DN (2008) Chronic depression: update on classification and
treatment. Current psychiatry reports 10: 458–464.
21. Belmaker RH, Agam G (2008) Major depressive disorder. The New England
49. Sahay A, Hen R (2007) Adult hippocampal neurogenesis in depression. Nature
journal of medicine 358: 55–68. doi: 10.1056/nejmra073096.
neuroscience 10: 1110–1115. doi:10.1038/nn1969.
22. Lopez-Munoz F, Alamo C (2009) Monoaminergic Neurotransmission: The
50. Cheng S (2013) The CRISP theory of hippocampal function in episodic
History of the Discovery of Antidepressants from 1950s Until Today. Current
memory. Frontiers in neural circuits 7: 88. doi:10.3389/fncir.2013.00088.
Pharmaceutical Design 15: 1563–1586. doi:10.2174/138161209788168001.
51. Spijker J, de Graaf R, Bijl R, Beekman A, Ormel J, et al. (2002) Duration of
23. Morilak DA, Frazer A (2004) Antidepressants and brain monoaminergic
major depressive episodes in the general population: results from The
systems: a dimensional approach to understanding their behavioural effects in
Netherlands Mental Health Survey and Incidence Study (NEMESIS). The
depression and anxiety disorders. The international journal of neuropsycho-
British journal of psychiatry: the journal of mental science 181: 208–213. doi:
pharmacology/official scientific journal of the Collegium Internationale
Neuropsychopharmacologicum (CINP) 7: 193–218. doi:10.1017/
52. Furukawa TA, Kitamura T, Takahashi K (2000) Time to recovery of an
inception cohort with hitherto untreated unipolar major depressive episodes.
24. Santarelli L, Saxe M, Gross C, Surget A, Battaglia F, et al. (2003) Requirement
The British journal of psychiatry: the journal of mental science 177: 331–335.
of hippocampal neurogenesis for the behavioral effects of antidepressants.
53. Angst J, Preisig M (1995) Course of a clinical cohort of unipolar, bipolar and
Science (New York, NY) 301: 805–809. doi: 10.1126/science.1083328.
schizoaffective patients. Results of a prospective study from 1959 to 1985.
25. Thompson C (2002) Onset of action of antidepressants: results of different
Schweizer Archiv fu¨r Neurologie und Psychiatrie (Zurich, Switzerland: 1985)
analyses. Human psychopharmacology 17 Suppl 1: S27–32. doi:10.1002/
146: 5–16.
54. Keller MB, Shapiro RW, Lavori PW, Wolfe N (1982) Recovery in major
26. Stassen HH, Delini-Stula A, Angst J (1993) Time course of improvement under
depressive disorder: analysis with the life table and regression models. Archives
antidepressant treatment: A survival-analytical approach. European Neuropsy-
of general psychiatry 39: 905–910.
chopharmacology 3: 127–135. doi:10.1016/0924-977X(93)90264-M.
55. Solomon DA, Keller MB, Leon AC, Mueller TI, Shea MT, et al. (1997)
27. Segman RH, Gorfine M, Lerer B, Shapira B (1995) Onset and time course of
Recovery from major depression. A 10-year prospective follow-up across
antidepressant action: psychopharmacological implications of a controlled trial
multiple episodes. Archives of general psychiatry 54: 1001–1006.
of electroconvulsive therapy. Psychopharmacology 119: 440–448. doi:10.1007/
56. Mueller TI, Keller MB, Leon AC, Solomon DA, Shea MT, et al. (1996)
Recovery after 5 years of unremitting major depressive disorder. Archives of
28. Quitkin FM, Stewart JW, McGrath PJ, Nunes E, Ocepek-Welikson K, et al.
general psychiatry 53: 794–799.
(1993) Further evidence that a placebo response to antidepressants can be
57. Beck JS (1995) Cognitive therapy: Basics and Beyond. New York: Guilford Press.
identified. The American journal of psychiatry 150: 566–570.
58. Hollon SD, Thase ME, Markowitz JC (2002) Treatment and Prevention of
29. Machado-Vieira R, Salvadore G, Luckenbaugh DA, Manji HK, Zarate CA
Depression. Psychological Science in the Public Interest 3: 39–77. doi:10.1111/
(2008) Rapid onset of antidepressant action: a new paradigm in the research and
treatment of major depressive disorder. The Journal of clinical psychiatry 69:
59. Jarrett RB, Schaffer M, McIntire D, Witt-Browder A, Kraft D, et al. (1999)
Treatment of atypical depression with cognitive therapy or phenelzine: a double-
30. Macedo-Soares MB de, Moreno RA, Rigonatti SP, Lafer B (2005) Efficacy of
blind, placebo-controlled trial. Archives of general psychiatry 56: 431–437.
electroconvulsive therapy in treatment-resistant bipolar disorder: a case series.
60. Hollon SD, DeRubeis RJ, Evans MD, Wiemer MJ, Garvey MJ, et al. (1992)
The journal of ECT 21: 31–34.
Cognitive therapy and pharmacotherapy for depression. Singly and in
31. Ruhe´ H, Huyser J, Swinkels J, Schene A (2006) Switching antidepressants after a
combination. Archives of general psychiatry 49: 774–781.
first selective serotonin reuptake inhibitor in major depressive disorder: a
61. Dunn AL, Trivedi MH, Kampert JB, Clark CG, Chambliss HO (2005) Exercise
systematic review. The Journal of clinical psychiatry 67: 1836–1855.
treatment for depression: efficacy and dose response. American journal of
32. Walsh BT, Seidman SN, Sysko R, Gould M (2002) Placebo Response in Studies
preventive medicine 28: 1–8. doi:10.1016/j.amepre.2004.09.003.
of Major Depression. JAMA 287: 1840. doi:10.1001/jama.287.14.1840.
62. Blumenthal JA, Babyak MA, Doraiswamy PM, Watkins L, Hoffman BM, et al.
33. Anderson IM, Tomenson BM (1994) The efficacy of selective serotonin re-
(2007) Exercise and pharmacotherapy in the treatment of major depressive
uptake inhibitors in depression: a meta-analysis of studies against tricyclic
disorder. Psychosomatic medicine 69: 587–596. doi:10.1097/PSY.0-
antidepressants. Journal of psychopharmacology (Oxford, England) 8: 238–249.
63. Martinsen EW (2008) Physical activity in the prevention and treatment of
34. Fava M (2000) New approaches to the treatment of refractory depression. The
anxiety and depression. Nordic journal of psychiatry 62 Suppl 4: 25–29.
Journal of clinical psychiatry 61 Suppl 1: 26–32.
35. Nelson JC (1998) Treatment of antidepressant nonresponders: augmentation or
64. Siegle G, Thompson W, Carter C, Steinhauer S, Thase M (2007) Increased
switch? The Journal of clinical psychiatry 59 Suppl 1: 35–41.
amygdala and decreased dorsolateral prefrontal BOLD responses in unipolar
36. Kirsch I, SG (1998) Listening to prozac but hearing placebo: a meta-analysis of
depression: related and independent features. Biological psychiatry 61: 198–209.
antidepressant medicatione. Prevention and treatment article 0002a I, article.
doi: doi: 10.1016/j.biopsych.2006.05.048.
37. Ellis HC, Ottaway SA, Varner LJ, Becker AS, Moore BA (1997) Emotion,
65. Surguladze S, Brammer M, Keedwell P, Giampietro V, Young A, et al. (2005) A
motivation, and text comprehension: the detection of contradictions in passages.
differential pattern of neural response toward sad versus happy facial expressions
Journal of experimental psychology General 126: 131–146.
in major depressive disorder. Biological psychiatry 57: 201–209. doi: 10.1016/
38. Thase ME (1999) How should efficacy be evaluated in randomized clinical trials
of treatments for depression? The Journal of clinical psychiatry 60 Suppl 4: 23–
66. Drevets W, Bogers W, Raichle M (2002) Functional anatomical correlates of
31; discussion 32.
antidepressant drug treatment assessed using PET measures of regional glucose
39. Perry R, Cassagnol M (2009) Desvenlafaxine: a new serotonin-norepinephrine
metabolism. European neuropsychopharmacology: the journal of the European
reuptake inhibitor for the treatment of adults with major depressive disorder.
College of Neuropsychopharmacology 12: 527–544.
Clinical therapeutics 31 Pt 1: 1374–1404. doi:10.1016/j.clinthera.2009.07.012.
67. Hamilton P, Gotlib I (2008) Neural substrates of increased memory sensitivity
40. Nemeroff CB, Heim CM, Thase ME, Klein DN, Rush a J, et al. (2003)
for negative stimuli in major depression. Biological psychiatry 63: 1155–1162.
Differential responses to psychotherapy versus pharmacotherapy in patients with
chronic forms of major depression and childhood trauma. Proceedings of the
68. Ramel W, Goldin P, Eyler L, Brown G, Gotlib I, et al. (2007) Amygdala
National Academy of Sciences of the United States of America 100: 14293–
reactivity and mood-congruent memory in individuals at risk for depressive
relapse. Biological psychiatry 61: 231–239. doi: 10.1016/j.biopsych.2006.
41. Beck AT (1976) Cognitive therapy and the emotional disorders.
42. Moore MT, Fresco DM (2012) Depressive realism: a meta-analytic review.
69. Widiger TA, Samuel DB (2005) Diagnostic categories or dimensions? A question
Clinical psychology review 32: 496–509. doi:10.1016/j.cpr.2012.05.004.
for the Diagnostic And Statistical Manual Of Mental Disorders–fifth edition.
43. DeRubeis RJ, Crits-Christoph P (1998) Empirically supported individual and
Journal of abnormal psychology 114: 494–504. doi:10.1037/0021-
group psychological treatments for adult mental disorders. Journal of consulting
and clinical psychology 66: 37–52.
70. Edwards VJ, Holden GW, Felitti VJ, Anda RF (2003) Relationship between
44. Kennedy SH (2008) Core symptoms of major depressive disorder: relevance to
multiple forms of childhood maltreatment and adult mental health in
diagnosis and treatment. Dialogues in clinical neuroscience 10: 271–277.
community respondents: results from the adverse childhood experiences study.
45. Frank E, Prien RF, Jarrett RB, Keller MB, Kupfer DJ, et al. (1991)
The American journal of psychiatry 160: 1453–1460.
Conceptualization and rationale for consensus definitions of terms in major
71. Chapman DP, Whitfield CL, Felitti VJ, Dube SR, Edwards VJ, et al. (2004)
depressive disorder. Remission, recovery, relapse, and recurrence. Archives of
Adverse childhood experiences and the risk of depressive disorders in adulthood.
general psychiatry 48: 851–855.
Journal of affective disorders 82: 217–225. doi:10.1016/j.jad.2003.12.013.
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Modeling the Dynamics of Disease States in Depression
72. Heim C, Newport DJ, Mletzko T, Miller AH, Nemeroff CB (2008) The link
80. Geddes JR, Carney SM, Davies C, Furukawa T a, Kupfer DJ, et al. (2003)
between childhood trauma and depression: insights from HPA axis studies in
Relapse prevention with antidepressant drug treatment in depressive disorders: a
humans. Psychoneuroendocrinology 33: 693–710. doi:10.1016/j.psyneuen.
systematic review. Lancet 361: 653–661. doi:10.1016/S0140-6736(03)12599-8.
81. Furukawa T a (2000) Time to recovery of an inception cohort with hitherto
73. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, et al. (1998)
untreated unipolar major depressive episodes. The British Journal of Psychiatry
Relationship of childhood abuse and household dysfunction to many of the
177: 331–335. doi:10.1192/bjp.177.4.331.
leading causes of death in adults. The Adverse Childhood Experiences (ACE)
82. Mueller TI, Leon a C, Keller MB, Solomon D a, Endicott J, et al. (1999)
Study. American journal of preventive medicine 14: 245–258.
Recurrence after recovery from major depressive disorder during 15 years of
74. Gladstone GL, Parker GB, Mitchell PB, Malhi GS, Wilhelm K, et al. (2004)
observational follow-up. The American journal of psychiatry 156: 1000–1006.
Implications of childhood trauma for depressed women: an analysis of pathways
83. Keller MB, Lavori PW, Rice J, Coryell W, Hirschfeld RM (1986) The persistent
from childhood sexual abuse to deliberate self-harm and revictimization. The
risk of chronicity in recurrent episodes of nonbipolar major depressive disorder:
American journal of psychiatry 161: 1417–1425. doi:10.1176/appi.ajp.
a prospective follow-up. The American journal of psychiatry 143: 24–28.
84. Andrade L, Caraveo-Anduaga JJ, Berglund P, Bijl RV, De Graaf R, et al. (2003)
75. Bernet CZ, Stein MB (1999) Relationship of childhood maltreatment to the
The epidemiology of major depressive episodes: results from the International
onset and course of major depression in adulthood. Depression and anxiety 9:
Consortium of Psychiatric Epidemiology (ICPE) Surveys. International journal
of methods in psychiatric research 12: 3–21.
76. Zlotnick C, Mattia J, Zimmerman M (2001) Clinical features of survivors of
85. Consensus Development Panel (1985) NIMH/NIH Consensus Development
sexual abuse with major depression. Child abuse & neglect 25: 357–367.
Conference statement. Mood disorders: pharmacologic prevention of recur-
77. Zlotnick C, Ryan CE, Miller IW, Keitner GI (1995) Childhood abuse and
rences. Consensus Development Panel. American Journal of Psychiatry 142:
recovery from major depression. Child abuse & neglect 19: 1513–1516.
78. Hayden EP, Klein DN (2001) Outcome of dysthymic disorder at 5-year follow-
86. Luty SE, Carter JD, McKenzie JM, Rae AM, Frampton CMA, et al. (2007)
up: the effect of familial psychopathology, early adversity, personality,
Randomised controlled trial of interpersonal psychotherapy and cognitive-
comorbidity, and chronic stress. The American journal of psychiatry 158:
behavioural therapy for depression. The British journal of psychiatry: the journal
of mental science 190: 496–502. doi:10.1192/bjp.bp.106.024729.
79. Kaplan MJ, Klinetob NA (2000) Childhood emotional trauma and chronic
87. Mo¨ller HJ, Mu¨ller H, Volz HP (1996) How to assess the onset of antidepressant
posttraumatic stress disorder in adult outpatients with treatment-resistant
effect: comparison of global ratings and findings based on depression scales.
depression. The Journal of nervous and mental disease 188: 596–601.
Pharmacopsychiatry 29: 57–62. doi:10.1055/s-2007-979545.
PLOS ONE www.plosone.org
October 2014 Volume 9 Issue 10 e110358
Source: https://www.stiftung-mercator.de/media/downloads/3_Publikationen/Demic_Cheng_Modeling_the_Dynamics_of_Disease_States_in_Depression.pdf
Solving the Internet gridlock : Daily-cardinal Web Search powered by Y A HO O ! SEA RC H Solving the Internet gridlock November 13, 2008 12:00 am • During high school, my home computer was so mind-numbingly slow that I would click on AOL, go downstairs, make a sandwich, eat it and return just as it asked me to log in. I did this until I could no longer stomach the thought of using it again and bought a Mac. Less than two years
dans le traitement des Maladies InflammatoiresChroniques de l'Intestin • Maladie de Crohn • Rectocolite Hémorragique l'effet est obtenu, on diminue peu à peu la dose, en faisant des "paliers" de 10 Cette fiche rédigée en 2005 par ou 5 mg, chaque semaine. Il ne faut pas interrompre un traitement corticoïde les gastro-entérologues spécialistes du GETAID