Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Urologists.co.uk
Postgrad Med J 2007;83:469–472. doi: 10.1136/pgmj.2006.055913
The diagnostic approach to ureteric colic has changed due to
ultrasound, intravenous urography and computed
the introduction of new radiological imaging such as non-
contrast CT. The role of intravenous urography, which is
Plain radiograph of the kidney, ureter and
regarded as the gold standard for the diagnosis of ureteric
colic, is being challenged by CT, which has become the first-line A plain radiograph of the kidney, ureter and
bladder (KUB) has a sensitivity that ranges from
investigation in a number of centres. The management of
45–60% in the evaluation of acute flank pain.2
ureteric colic has also changed. The role of medical treatment
Overlaying bowel gas or stool (faecoliths) and
has expanded beyond symptomatic control to attempt to target abdominal or pelvic calcifications (phleboliths) can
make identification of ureteric stones difficult. In
some of the factors in stone retention and thereby improve the addition, a KUB cannot visualise radiolucent
likelihood of spontaneous stone expulsion.
stones (10–20% of stones), thus limiting the value
of plain radiography. However, a KUB may sufficefor assessing the size, shape, and location ofurinary calculi in some patients (fig 1).
Ureteric colic is an important and frequent
emergency in medical practice. It is most
commonly caused by the obstruction of the
Ultrasonography allows direct demonstration of
urinary tract by calculi. Between 5–12% of the
urinary stones located at the PUJ, the VUJ, and in
population will have a urinary tract stone during
the renal pelvis or calyces.3 Stones located between
their lifetime, and recurrence rates approach 50%.1
the PUJ and VUJ, however, are extremely difficultto visualise with ultrasonography.
CLINICAL PRESENTATIONThe classic presentation of a ureteric colic is acute,
Intravenous urography
colicky flank pain radiating to the groin. The pain
Since it was first performed in 1923, intravenous
is often described as the worst pain the patient has
urography (IVU) has been the traditional ‘‘gold
ever had experienced. Ureteric colic occurs as a
standard'' in the evaluation in ureteric colic. It
result of obstruction of the urinary tract by calculi
provides structural and functional information,
at the narrowest anatomical areas of the ureter:
including site, degree and nature of obstruction.
the pelviureteric junction (PUJ), near the pelvic
Whereas IVU has a detection rate as high as 70–
brim at the crossing of the iliac vessels and the
90% (fig 2),4 it can only visualise radiopaque
narrowest area, the vesicoureteric junction (VUJ).
stones (80–90% of stones). Despite its usefulness,
Location of pain may be related but is not an
there are some undesirable aspects of IVU, includ-
accurate prediction of the position of the stone
ing radiation exposure, risk of nephrotoxicity,
within the urinary tract. As the stone approaches
contrast reaction and the time it takes, particularly
the vesicoureteric junction, symptoms of bladder
when delayed films are required.
irritability may occur.
Calcium stones (calcium oxalate, calcium phos-
The reported incidence of contrast-induced renal
phate and mixed calcium oxalate and phosphate)
failure is approximately 1%,5 while in the popula-
are the most common type of stone, while up to
tion with pre-existing renal failure and diabetes
20% of cases present with uric acid, cystine and
mellitus, the risk of contrast-induced nephrotoxi-
struvite stones.
Physical examination typically shows a patient
Metformin is an oral agent, used in the manage-
who is often writhing in distress and pacing about
ment of diabetes mellitus. Metformin is excreted
trying to find a comfortable position; this is, in
unmetabolised by the kidney. It is not nephrotoxic;
contrast to a patient with peritoneal irritation who
See end of article for
however, a major concern is the potential hazard
authors' affiliations
of metformin-induced lactic acidosis in those who
Tenderness of the costovertebral angle or lower
develop contrast-induced oliguria. In this setting,
quadrant may be present. Gross or microscopic
Correspondence to:
metformin can accumulate, resulting in the sub-
haematuria occurs in approximately 90% of
Dr M Masarani, 18 St
sequent accumulation of lactic acid. Metformin-
Peter's Way, London W5
patients; however, the absence of haematuria does
induced lactic acidosis is fatal in half of the
2QR, UK; mmasaarane@
not preclude the presence of stones.
Abbreviations: CT, computed tomography; IVU,
intravenous urography; KUB, plain radiograph of the
Besides routine history and clinical examination,
kidney, ureter and bladder; MET, medical expulsive
Accepted 25 January 2007
investigations of patients with suspected ureteric
therapy; NSAIDs, non-steroidal anti-inflammatory drugs;
PUJ, pelviureteric junction; VUJ, vesicoureteric junction

Masarani, Dinneen
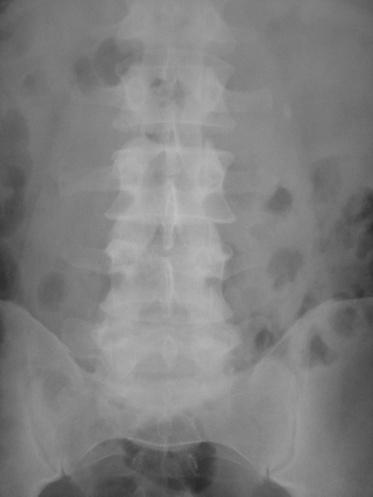
Figure 1 Patient presented with left loin pain. Kidney, ureter and bladder
Figure 2 Patient after administration of intravenous contrast medium,
(KUB) x ray showing 7 mm radiopaque stone laying lateral to the tip of
showing left nephrogram and contrast coming down to the level of the
transverse process of L2.
affected patients; however, it is a very rare complication.7
incidence of extra-urinary abnormality with CT is 6–12%.11
In patients with normal renal function metformin should be
Those reported abnormalities include pelvic inflammatory
discontinued at the time of the IVU and withheld for the
disease, adnexal masses, tubo-ovarian abscess, appendicitis,
subsequent 48 h. For patients with abnormal renal function,
diverticulitis, cholecystitis, pancreatitis or unexpected malig-
metformin should similarly be discontinued at the time of the
nancy. In some cases, intravenous contrast medium will be
IVU and only be reinstated when renal function has been re-
necessary for further characterisation of any of the unexpected
evaluated and found to be normal.8
Contrast reaction
Disadvantages of CT
In the general population the incidence of contrast reaction is
An important limitation of CT is the fact that it does not permit
5–10%, including mild reactions such as vomiting and urticaria,
functional evaluation of the kidneys and it is unable to assess
as well as more serious reactions such as bronchospasm and
the degree of obstruction. The presence of a stone does not
anaphylaxis (the risk of anaphylaxis is 157 per 100 000).9 The
necessarily mean that the kidney is obstructed. The relative lack
incidence of contrast reaction can be diminished in many cases
of functional information derived from CT, compared with the
with the use of expensive low osmolar contrast agents but it
renal excretory times evident during IVU, might compromise
cannot be entirely eliminated.
clinical management. However, some authors have suggestedthat secondary features of obstruction on CT which include
Non-contrast enhanced computed tomography
hydronephrosis, hydroureter, renal enlargement and inflam-
Unenhanced computed tomography (CT) provides an increas-
matory changes of the perirenal fat, that are referred to as
ingly popular alternative for evaluating ureteric colic.
perinephric stranding, are a reliable parallel of delayedexcretion on IVU.12
Another major disadvantage of CT is the higher radiation
CT has the following advantages over IVU: it has higher
exposure of the patient compared with KUB or IVU. CT in this
sensitivity and specificity for calculus detection, it does not use
setting requires at least three times the radiation exposure of
intravenous contrast medium, it permits alternative diagnoses,
IVU and 10 times that of abdominal radiography and presents
and requires a shorter examination time.
an additional lifetime risk of malignancy of 1 in 4000.13 Newer
The accuracy of non-contrast CT in detecting stone disease
protocols involving reduced radiation exposure without com-
has been indisputable with sensitivity, specificity and positive
promising efficacy are developing and are likely to reduce
predictive value of CT being reported as 96%, 100% and 100%,
further the radiation exposure from CT (table 1). Low-dose and
respectively.10 CT can visualise all radiopaque stones, as well as
ultra low-dose CT reduced radiation exposure by about 50% and
radiolucent stones such as uric acid and cystine calculi (fig 3).
95%, respectively, compared with standard-dose CT, with
When CT confirms the presence of a stone, a plain abdominal
comparable detection rates of calculi and non-stone-associated
radiograph should be obtained to assess whether the stone is
abnormalities (table 2).14 15
radiopaque. This is helpful as only the KUB radiograph is
Another disadvantage is that CT services are not universally
needed later to determine if the stone has moved or passed.
available for 24 h period and a radiologist may be required for
Avoiding the use of intravenous contrast medium is perhaps
the accurate interpretation of the films.
the most distinct benefit of CT in this situation.
Finally, in the current healthcare climate, cost and avail-
CT also provides an opportunity to identify extra-urinary
ability will always be central factors determining the use of CT
pathology during the primary investigation of patients in whom
in the acute setting. A frequent criticism of CT is that it costs
a definitive diagnosis is not always apparent. The reported
more than IVU. However, when taking into account the

Table 1 Radiation exposure of different imagingmodalities
Radiation exposure (mSv)
Ultra-low dose CT
CT, computed tomography; IVU, intravenous urography; KUB,plain radiograph of the kidney, ureter and bladder.
these drugs to be as effective as opioids, with the latter used asrescue medications.18 Opioids have higher rates of nausea,vomiting, and dizziness.
Data on the effect of opiates on ureteric tone suggest that
they cause an increase or no change in tone. Opiate-seekingpatients might therefore spuriously present with symptoms ofureteric colic.
NSAIDs block prostaglandin-induced effects. They also
reduce local oedema and inflammation, and inhibit thestimulation of ureteric smooth muscle, which is responsiblefor increased peristalsis and subsequently increased uretericpressure. Although NSAIDs reduce pain associated withureteric colic, they may potentially interfere with the kidney'sautoregulatory response to obstruction by reducing renal bloodflow, and renal failure may be induced with pre-existing renaldisease. The choice of agent is generally based on clinicianpreference, personal experience and institutional culture.
Medical expulsive therapyThe traditional treatment indicated above has recently beenimproved by the application of active medical expulsive therapy(MET). Protocols were developed based on the possible causes
Figure 3 Non-contrast computed tomography (CT) showing right
vesicoureteric junction (VUJ).
of failure to pass a stone spontaneously, including muscle
advantage of reduced expenditure in terms of time and
Table 2 Intravenous urography (IVU) versus computed
manpower for CT, it is suggested that indirect costs are much
lower for CT scans.16
Indisputable accuracy
Given that most ureteric stones will pass spontaneously,conservative treatment in the form of observation with
Risk of nephrotoxicity or
No intravenous contrast is
dangerous reaction to
necessary so no risk of
analgesia is the preferred approach. Ureteric stones require
intravenous contrast medium
nephrotoxicity or contrast
radiological or surgical intervention only when the conservative
treatment fails. The probability of spontaneous passage is basedon a number of factors including stone size, stone position,
Cannot be used in azotemia
or known significant allergy to
degree of impaction and degree of obstruction. The likelihood of
intravenous contrast agents
spontaneous stone passage decreases as the size of the stoneincreases (table 3).17 Most authors recommend that stone
Less radiation dose
Standard CT requires at
passage should not exceed 4–6 weeks due to the risk of renal
least three times the
radiation exposure of IVU
Hard to see radiolucent stones, With only rare exceptions
although indirect signs of
it shows all stones clearly
The pain of ureteric colic is due to obstruction of urinary flow,
obstruction may be apparent
with a subsequent increase in wall tension. Rising pressure inthe renal pelvis stimulates the local synthesis and release of
Shows relative kidney function Does not give functional
prostaglandins, and subsequent vasodilatation induces a diur-esis which further increases intrarenal pressure. Prostaglandins
Ureteric kinks, strictures or
also act directly on the ureter to induce spasm of the smooth
tortuosities are often visible
muscle. Owing to the shared splanchnic innervation of the
Cannot be used to evaluate
Demonstrates other
renal capsule and intestines, hydronephrosis and distension of
the renal capsule may produce nausea and vomiting.
Relatively slow, may need
multiple delay films, which
The choice of analgesia used in the management of acute
ureteric colic is changing, with increasing use of non-steroidalanti-inflammatory drugs (NSAIDs). Most studies have shown
Masarani, Dinneen
. . . . . . . . . . . .
Authors' affiliations
Table 3 Likelihood of passage of ureteric stones17
M Masarani, M Dinneen, Department of Urology, Imperial College
London, Chelsea & Westminster Teaching Hospital, London, UK
spontaneous passage (%)
Conflict of interest: none stated
1 Sierakowski R, Finlayson B, landes RR, et al. The frequency of urolithiasis in
hospital discharge diagnoses in the United States. Invest Urol 1978;15:438–41.
2 Mutgi A, Williams JW, Nettleman M. Renal colic: utility of the plain abdominal
roentgenogram. Arch Intern Med 1991;151:1589–92.
3 Sheafor DH, Hertzberg BS, Freed KS, et al. Non-enhanced helical CT and US in
spasm, local oedema, inflammation, and infection. Regimens
the emergency evaluation of patients with renal colic: prospective comparison.
have commonly included a corticosteroid (to reduce local
oedema through its anti-inflammatory action), antibiotics (to
4 Miller OF, Rineer SK, Reichard SR, et al. Prospective comparison of unenhanced
spiral computed tomography and intravenous urogram in the evaluation of acute
prevent or treat urinary tract infection), as well as calcium
flank pain. Urology 1998;52:982–7.
antagonists and a-blockers (agents directed towards stone-
5 Levy EM, Viscolli CM, Horwitz RI. The effect of acute renal failure on mortality: A
induced ureteric spasm). Combination therapy is intended for
cohort analysis. JAMA 1996;275:1489–94.
6 Barrett BJ, Carlisle EJ. Meta analysis of the relative nephrotoxicity of high- and
short-term use.
low-osmolality iodinated contrast media. Radiology 1993;188:171–5.
7 Thompson NW, Thompson TJ, Love MHS, et al. Drugs and intravenous media.
NSAID: NSAIDs have ureteric-relaxing effects and, as such,
BJU Int 2000;85:219–21.
can be considered to be a form of MET; yet the only
8 Royal College of Radiologists. Royal College of Radiologists' guidelines with
randomised, double blinded, placebo-controlled trial showed
regard to metformin-induced lactic acidosis and x-ray contrast medium agents.
London: The Royal College of Radiologists, 1999;99:2.
no difference in augmenting stones passage between
9 Shehadi WM, Toniolo G. Adverse reactions to contrast media: a report from the
NSAIDs and placebo.19
Committee on Safety of Contrast Media of the International Society of Radiology.
N Calcium antagonists: Ureteric smooth muscle uses an
10 Worster A, Preyra I, Weaver B, et al. The accuracy of noncontrast helical
active calcium channel pump in order to contract. Calcium
computed tomography versus intravenous pyelography in the diagnosis of
antagonists suppress the fast component of ureteric con-
suspected acute urolithiasis: a meta-analysis. Ann Emerg Med 2002;40:280–6.
traction, leaving peristaltic rhythm unchanged. Therefore
11 Ahmad NA, Ather MH, Rees J. incidental diagnosis of disease on un-enhanced
helical computed tomography performed for ureteric colic. BMC Urol
calcium channel blockers, which are commonly used in the
treatment of hypertension and angina, have been used to
12 Smith RC, Verga M, Dalrymple N, et al. Acute ureteral obstruction: value of
relax ureteric smooth muscle and enhance stone passage.20
secondary signs of obstruction of the urinary tract on unenhanced helical CT.
Am J Roentgenol 1996;167:1109–13.
a-Blockers: a1-Adrenergic antagonists are currently com-
13 Denton ER, Mackenzie A, Greenwell T, et al. Unenhanced helical CT for renal
monly used as first-line treatment in men with lower urinary
colic: is the radiation dose justifiable? Clin Radiol 1999;54:444–7.
tract symptoms. Both a and b adrenoreceptors have been
14 Meagher T, Sukumar VP, Collingwood J, et al. Low-dose computed tomography
shown to exist within the ureter, particularly in the lower
in suspected acute renal colic. Clin Radiol 2001;56:873–6.
15 Kluner C, Hein PA, Gralla MD, et al. Does ultra-low-dose CT with a radiation
and intramural portions. a1-Adrenergic antagonists inhibit
dose equivalent to that of KUB suffice to detect renal and ureteral calculi? Comput
the basal tone, peristaltic wave frequency and the ureteric
Assist Tomogr 2006;30:44–50.
contraction in the intramural parts. As a result the
16 Pfister SA, Deckart A, Laschke S, et al. Unenhanced helical computed
tomography vs intravenous urography in patients with acute flank pain: accuracy
intraureteric pressure below the stone decreases and
and economic impact in a randomized prospective trial. Eur Radiogr
elimination of the stone can be achieved.21
17 Miller OF, Kane CJ. Time to stone passage for observed ureteral calculi: a guide
Patients treated with calcium antagonists or a-blockers had a
to patient education. J Urol 1999;162:688–90.
65% greater likelihood of spontaneous stone passage than
18 Holdgate A, Pollock T. Nonsteroidal anti-inflammatory drugs versus opioids for
acute renal colic. Cochrane Database Syst Rev 2004;(1):CD004137.
patients not given these drugs. Calcium-channel blockers and
19 Laerum E, Ommundsen OE, Gronseth JE, et al. oral diclofenac in the
a-blockers seemed well tolerated.22–25
prophylactic treatment of recurrent renal colic. A double-blind comparison with
The addition of corticosteroids might have a small advantage
placebo. Eur Urol 1995;28:108–11.
but the benefit of drug therapy is not lost in those patients for
20 Salman S, Castilla C, Vela NR. Action of calcium antagonists on ureteral
dynamics. Actas Urol Esp 1989;13:150–2.
whom corticosteroids might be contraindicated.26–28
21 Sigala S, Dellabella M, Milanese G, et al. Evidence for the presence of a 2
There are additional benefits which seem to be associated
adrenoceptor subtypes in the human ureter. Neurourol Urodyn 2005;24:142–8.
with MET. Patients have a significantly reduced time to stone
22 Porpiglia F, Destefanis P, Fiori C, et al. Effectiveness of nifedipine and defluzacort
in the management of distal ureteral stones. Urology 2000;56:579–83.
passage, significantly fewer pain episodes, lower analogue pain
23 Dellabella M, Milanese G, Muzzonigro G. Efficacy of tamsulosin in the medical
scores, and need significantly lower doses of analgesics.
management of juxtavesical ureteral stones. J Urol 2003;170:2202–5.
When conservative therapy fails, the choice of treatment lies
24 Dellabella M, Milanses G, Muzzonigro G. Randomized trial of the efficacy of
between shock wave lithotripsy and ureteroscopy. Surgical
tamsulosin, nifedipine and phloroglucinol in medical expulsive therapy for distalureteral calculi. J Urol 2005;174:167–72.
management is beyond the scope of this article and it is not
25 Hollingsworth JM, Rogers MAM, Kaufman S, et al. medical therapy to facilitate
discussed here.
urinary stones passage: a meta analysis. Lancet 2006;368:1171–9.
26 Dellabella M, Milanses G, Muzzonigro G. medical expulsive therapy for distal
ureterolithiasis: Randomized prospective study on the role of corticosteroids usedin combination with tamsulosin-simplified treatment regimen and health-related
Acute ureteric colic is a common surgical emergency. There is a
quality of life. 2005;66:712–15.
shift towards using non-contrast CT in evaluating ureteric colic.
27 Salehi M, Fouladi MM, Shier H, et al. Does methylprednisolone acetate increase
MET has shown promise in increasing the spontaneous stone
the success rate of medical therapy for patients with distal ureteral stones. EurUrol Suppl 2005;4:24–8.
passage rate and relieving discomfort while minimising
28 Pearle MS. Comment on medical therapy to facilitate urinary stones passage.
narcotic usage.
Source: http://urologists.co.uk/wp-content/uploads/2016/04/Ureteric-colic.pdf
Vol 38, No 3, September 2013 Effect of Medium pH on Antibiotic Activity against Syrian Brucella spp. Isolates Ayman Al-Mariri, PhD; Mazen Safi, PhD Abstract Background: Brucellosis is an endemic zoonosis in Syria, affecting large numbers of animals. There are an increasing number of cases in humans. Brucella is a facultative intracellular
Documento descargado de http://www.elsevier.es el 10/03/2013. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato. Otras patologías esofágicas E. Pérez-Cuadrado y R. Gómez EspínUnidad Asistencial del Aparato Digestivo. Hospital Universitario Morales Meseguer. Murcia. España. - Anillos esofágicos