Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Untitled
JIMSA April-June 2012 Vol. 25 No. 2
Design and Development of Non Invasive Technique
for Diagnosis of Thyroid Disorders.
K. Jagadeesan, S.Muthan, R. Gomalavalli, K. Mohan Dass,
M.Chandrasekar, M. Paul Korath, T.M.R Panicker
Department of Surgery, K. J. Hospital & K. J. Research Foundation;
Department of ECE, Anna University; Department of Endocrine surgery, MMC/GGH, Chennai, India
Abstract: Functional abnormality of Thyroid as a common day today problem in clinical practices. Laser based light absorption techniques and
process used to create detection of thyroid diseases for clinical purposes. Laser plays a vital role in diagnosis status based on the reflectance [5] of
skin surface. Presently blood test is being done to find out the presence of thyroid hormones and confirming the presence of two main thyroidism.
The aim of this work is to classify thyroid status; Thyroid status is manifest in skin from the skin reflectance of the laser diode emission. From these
reflectance's thyroid is classified into Hyper and Hypothyroidism. Hence patients are benefited by providing detection and classification of thyroid
diseases prior to invasive lab test by puncturing the vein and collecting blood. As laser based technique has advantages of being non-invasive and
low cost in comparison to other diagnostic methods and it can be performed in a normal environment without any restriction. It is an idle tool for
mass screening to asses' thyroid status; this hypothesis was put forward by one of the authors namely K J.
difficulty in sleeping, a fast heartbeat, irregular menstrual periods ingirls, and muscle wasting weakness. People with hypoactive thyroids
Thyroid disease is due to the production abnormality of thyroid
might feel depressed and sluggish lethargic and Myxedema. Teens
hormones. Two major types of thyroidism are Hyperthyroidism
with hypothyroidism also might have slow growth in height, slow
(over production) and Hypothyroidism (low production). The
sexual development and irregular menstrual periods in girls, muscle
incident of Hypo thyroidism in the age group of 31-60yrs is 76.6%.
weakness, dry hair, poor memory, and difficulty in concentration.
the ratio of Female: male is 1:10. Hyperthyroidism is nearly 10 times
Thyroid stimulating hormone (TSH) promotes the growth of the
more frequent in women than in men. The thyroid gland is located in
thyroid gland in the neck and stimulates it to produce more thyroxin,
the lower front part of the neck. It produces thyroid hormones that
when there is an excessive amount of thyroid hormones, the pituitary
regulate the body's metabolism. It also plays a role in bone growth
gland stops producing TSH, where by reducing thyroid hormone
and development of the brain and nervous system in children. The
production. This mechanism maintains a relatively constant level of
pituitary gland controls the production of thyroid hormones. Thyroid
thyroid hormones circulating in the blood.
hormones also help to maintain normal blood, regulation of heart rate,digestion, muscle tone, and reproductive functions. The controlling
NEED FOR THE PROPOSED WORK
mechanism of endocrine system is the hypothalamus, pituitary,
Classification of thyroid status involves laser based light absorption
thyroid axis. The endocrine system is regulated by feedback in much
technique in a non invasive manner. Non invasive method of thyroid
the same way that a thermostat regulates the temperature in a room.
classification involves emission and reflectance of light. Most of this
For the hormones that are regulated by the pituitary gland, a signal is
detection work is based on light absorption. Generally, Emission of
sent from the hypothalamus to the pituitary gland in the form of a
light involves reflection, absorbance and scattering on the surfaces.
"releasing hormone", which stimulates the pituitary to secrete a
Observation of light absorbance by the receiver from the emitted
"stimulating hormone" into the circulation. The stimulating hormone
light classifies the hypo, eu & hyperthyroidism. The characteristics
signals the target gland to secrete hormones. As the level of this
of the thyroidism. The characteristics of the thyroidism and its
hormone rises in the circulation, the hypothalamus and the pituitary
symptoms were important features of the skin surfaces which are
gland shut down secretion of the releasing hormone and the stimulating
highly evaluated and had been differentiated.
hormone, which in turn slows the secretion by the target gland, thissytem results in stable blood concentrations of the hormones that are
MATERIAL AND METHODS
regulated by the pituitary gland. Hypothyroid state is also known as
This prospective study was carried out in 95 patients between the
Myxedema. Hyperthyroid is also known as Grave's disease and
age of 5-75 years in the department of endocrine and out patients list
Normal/treated thyroid status is called as Euthyroid.
in MMC & GH and KJH respectively from January to May 2010.
OVERVIEW OF THYROID
The thyroid diseases were classified into Hyperthyroid, Eu thyroidand Hypothyroid. The Hyperthyroid age ranged from 35-42 years.
The thyroid gland is located in the lower part of the neck, below the
All patients were carefully assessed as regards history, general
Adam's apple, wrapped around the trachea (windpipe). It has the
condition, systemic examination and conventional thyroidism
shape of a butterfly two wings (lobes) attached to one another by a
evaluation was done. Preliminary assessments were performed at
middle part. The thyroid secretes the thyroid hormones as thyroxin
KJH, Egmore with the patient's informed consent. Those unwilling
(T ) a tri-iodo-thyronine (T ) . These hormones regulate the rate of
patients, Diabetics and Uraemic patients were excluded from the
metabolism [4] affect the growth and rate of function of many other
study. The patients were divided into 3 groups. In group I, Hypo
systems in the body. The thyroid gland is controlled by the
patients of 20 were selected. In group II nearly 25 hyper patients
hypothalamus and pituitary gland. Hyperthyroidism can cause
were selected and in group III 30 Eu thyroid patients were selected.
nervous, irritability, increased perspiration, intolerance to heat, fatigue,
Correspondence: Dr. K. Jagadeesan, Chairman, K. J, Research Foundation, Director, K.J Hospitalt Research and PG Centre, 182, Poonamalle
HighRoad, Chennai -600084, India Fax: 044-26411886 e-mail: [email protected]

JIMSA April-June 2012 Vol. 25 No. 2
In each group, patients were investigated as BMI, age; T3, T4, TSH
Table.1: Subjects with EU Thyroidism
and results are tabulated. In our work it was identified by the skin
SUBJECTS between 1001 to 1021 count
surface reflectance [5] of the emitted laser diode. Laser Diode and sixphoto diodes were arranged in the cuff, in order to prevent the escapeof the reflected radiation. Depending on the characteristics of skinand tissue around the absorption and reflection vary.
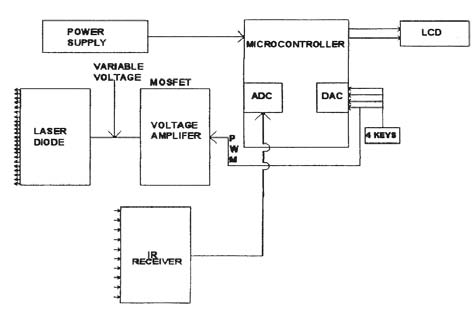
In our functional block diagram in figure A the characteristics of eachblock is well known labeled and its operation is performed by thePIC microcontroller for the analog and digital conversions for ourinput and output data transmission. The output is displayed by theLiquid crystal Display under programming of the microcontroller.
Laser diode is used to emit the light and the reflected light absorptionis detected by the infrared detectors, its particular value is displayedin LCD based on the count value the classification is done.
Hypo Thyroid Subjects
PlateA. Functional Block Diagram
Table. 2: Subjects with Hypo thyroidism
HYPO SUBJECTS <1000
Detected outputs were classified as Hyper/EU/Hyper thyroid's [2].
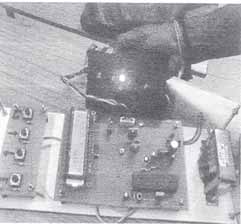
The entire setup was tried at room temperature. The cuff with thelaser diode and detectors fixed on the distal, anterior aspect of theforeman. The reading is measured within 2 seconds.
The emitted light from the laser was incident on the skin, their maybe absorbance, reflectance and scattering due to blood connectivetissues, epidermis and perilymph layer. The reflected light wascaptured by the detectors and their value is displayed in the LCD.
Based on the displayed count is shown in plate B.
Plate B: Display of LCDThe entire setup was tried on normal/hypo/hype/persons as pilotstudy and the readings are tabulated. More than 75 subjects weretaken and their counts are tabulated.
RESULTS AND DISCUSSIONS
In the table I and fig I represents the displayed outputs in terms ofcount for the hypo patients during the work.
The results acquired during the experimental setup are tabulated in
When TSH value increases and the count decreases. It is 1000 and
table I for Eu Thyroid Subjects.
X Axis: TSH datas & Y Axis: output count values
JIMSA April-June 2012 Vol. 25 No. 2
Table.4 Subjects with Hyper thyroidism SUBJECTS>=1022
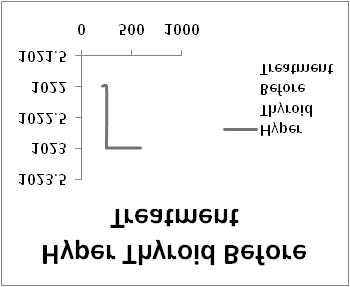
Fig 1: Correlation of TSH and Count of the subjectsTable. 3 Hypo Subjects On Treatment
The tabular column represents the patient status on treatment withdrugs thyroxine becomes Eu thyroid.
X Axis: TSH datas & Y Axis: output values
When there is increase in the T3/T4 value the response is increases inthe observing count value. In the table.4 lab values and the outputwere displayed in terms of count for the hyper patients during the
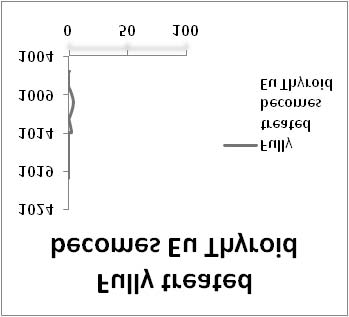
Fig 2 & 3 represents the flow for the patients on treatments by the
Thyroxine drugs.
X Axis: TSH datas & Y Axis: output count values
X Axis: T3/T4 datas & Y Axis: output count valuesIn the table 4 and fig 4 represents the displayed outputs in terms ofcount for the hyper patients during the work
X Axis:TSH datas; Y Axis:outputcount valuesFig. 2: Correlation of TSH andCount of the Subjects
X Axis:TSH datas; Y Axis:outputcount valuesFig. 3: Correlation of TSH andCount of the Subjects(reachedmargin level)
X Axis:T3/T4 datas ; Y Axis:output count valuesFig. 4: Correlation of T3/T4 and Count of the Subjects
HYPER THYROID SUBJECTS
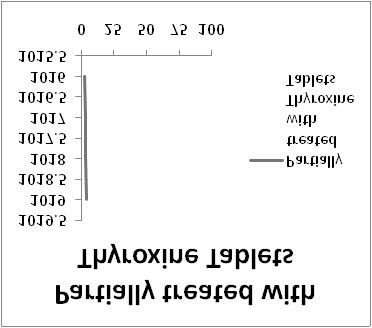
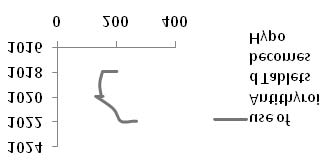
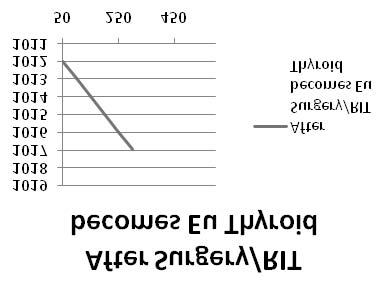
Fig 5 represents the count for the hyper patients after treatrment
Table.4 Subjects with Hyper thyroidism
with Antithyroid tablets and the flow represents the patient conditions
on treatment by the 6month were partially corrected .
JIMSA April-June 2012 Vol. 25 No. 2
Table. 5 Hyper Subjects On Treatment
Table.5: Subjects with Hypo thyroidism HYPO SUBJECTS <=1000
X Axis: T3/T4 datas & YAxis: output count valuesFig.6: Correlation of T3/T4and Count of the Subjects(reached margin level)
Fig 6 represents the count flow for the hyper patients on treatmentwith thyroxine after Thyroidectomy and Radio ablation Therapy(RAT) becomes Eu Thyroid.
Based on complexion we have undertaken readings to find out whetherthe pigment status, alters the reflectance value. The parameters age,sex, BMI and complexion has got no role in reflection of the laserphoto emission. But the TSH, T3 and T4values have a direct reflectionon the values.
Use of Antithyroid Tablets causes Hypo
To the volunteers at K J Hospital and MMC and the patients whovolunteered to join the study program. Special acknowledgement toMr. M.P.Vikraman for his help in evaluation of the equipment andpreparation of the article.
1. Azlee Zabidi, Wahidan Mansor, Lee Yoot Khuan, Rohilah Sahak and Frah Yasmin Abd Rahman (2009,'
Mel-Frequency cepstrum Coefficient Analysis of Infact Cry with Hypothyroidism', University Tech-nology Mara, IEEE Transaction on medical Imaging, Vol 4244, pp 204-208.
2. Cohen A., Wadsworth N. (1971),' A light emitting diode skin reflection oximeter',, Med. & bio. Engng,
Vol 10, pp 385-391.
3. Fatemeh Saiti, Afsareh Alavi Naini (2008),;Thyroid disease diagnosis based on genetic Algorithms
using PNN and SVM', Biomedical Engineering Group, K.N Toosi university of Technology, vol. 344(7),pp 501-509.
X Axis: T3/T4 datas & Y Axis: output count values
4. Gopakalova, Dubovik V, Khaziev V. and Misura E, (2006),' Influence of the lipid Metabolism of the
Fig.5: Correlation of T3/T4 and subjects Count
patients with primary hypothyroidism and ischemic heart disease', Academy of Medical Sciences ofUkraine 9IEPP), Vol.22, Issue 2, pp 165-169.
Fig 5 represents the flow for the hyper patients after treatment with
5. Maurizio Tobaldini, Nicola Montano, Albert Port and Milena Muratori (2008),' Increased complexity
of short term heart rate variability Hyperthyroid patients' during orthostatic challenge', Vol I, Issue 2,
Antithyroid drugs
pp 320-326.
A MILESTONE IN THE SERVICE OF THE COMMUNITY BY THE ROTARY CLUB OF DELHI CHANAKYAPURI (RI DISTRICT 3010)
In the year 1978, I was given the charge of the Physically Handicapped Committee of Rotary Club of Delhi Chanakyapuri as its Chairman by the thenPresident of the Club, Rtn. Raj Khullar. I comprehended that the term Physically Handicapped embraces a very vast array of challenging conditionslike visual, hearing, mobility etc., and therefore it would have been a futile attempt to address all of them. Therefore, it occurred to me that a dreadeddisease called Poliomyelitis was causing havoc to infants and children in Delhi resulting in large number of deaths and permanent paralytic disordersof the limbs in the surviving children. Although, there is, even to date, no medical cure available for this awful condition, an excellent oral vaccinehad been invented in Russia which offers total immunity from the disease. As a doctor, the dictum ‘Prevention is better than the Cure', is always inthe forefront of the mind. Thus I approached the then largest children's hospital in Delhi, the ‘Kalawati Saran Children's Hospital' and I was told thatthe Institution gets nearly 8,000 cases of Poliomyelitis every year from a nearby area in Pahargunj, New Delhi called Nabikarim. I proposed to offerthe services on behalf of the Community Service Avenue of the Rotary Club of Delhi Chanakyapuri in vaccinating the infants and children in theabove mentioned area which was the hotbed of poliomyelitis. This offer was immediately accepted by the authorities of the hospital who evenprovided some staff to help us conduct this marathon vaccination programme by going from door to door to motivate and vaccinate the infants andchildren. As is the case with all new drives, we met with resistance and suspicion. This did not deter us and we completed our job in 2–3 days.The result,a year later in 1979, the hospital reported only one case of Poliomyelitis from the same Nabikarim from where earlier thousands of cases used to comeevery year. On further enquiry we found that the affected baby's mother had hidden the infant from us when we came for administering the oralvaccine as she was apprehensive that it may cause some fatal side effects.
The Rotary International District 309 in 1980 recognised the efforts and awarded ‘Outstanding Rotarian' award to me during the District Conferenceheld at Srinagar, Kashmir in the year 1980. The Union Ministry of Health and Family Welfare also took cognizance of our efforts and appointed methe Honorary Advisor to the Ministry for their Polio Eradication Project for the year 1979–80. A point to highlight, if I may call it so, is that theRotary Club of Delhi Chanakyapuri thought of and executed the Polio Eradication years before the Rotary International Conceived the Idea. Nodoubt our effort was in a mini scale but it was a small beginning. I take this opportunity to thank the authorities of the Kalawati Saran Children'sHospital for the assistance extended to us.
PP Rtn Dr. Sandip Mukerjee, President (1985–86), Rotary Club of Delhi Chanakyapuri, RI District 3010.
Source: http://kjhospital.net/kjhospital/ViewArticle.aspx?qFileID=157
HUMAN GENE THERAPY 22:166–176 (February 2011)ª Mary Ann Liebert, Inc.DOI: 10.1089/hum.2010.099 Retroviral and Transposon-Based Tet-Regulated All-In-One Vectors with Reduced Background Expression and Improved Dynamic Range Niels Heinz,1 Axel Schambach,1 Melanie Galla,1 Tobias Maetzig,1 Christopher Baum,1 Rainer Loew,2 and Bernhard Schiedlmeier1 The regulated expression of therapeutic genes may become crucial in gene therapy when their constitutiveexpression interferes with cell fate in vivo. The efficient regulation of transgene expression requires tightly con-trolled inducible promoters, as shown for the tetracycline regulatory system (tet-system). However, its applicationrequires the introduction of two components into the target cell genome: the tet-responsive transactivator and theregulated expression cassette. In order to facilitate the usage of the tet-system for approaches in gene therapy, bothcomponents have to be transferred by a single vector, thus eliminating the preselection of transactivator positivecells. Published ‘‘all-in-one'' vectors for regulated transgene expression display a relatively low signal-to-noiseratio, resulting in regulatory windows of around 500-fold even in selected clones. In this study, we show that amodified vector architecture combined with the introduction of new tet-responsive promoters, Ptet, improved thedynamic range of such all-in-one vectors to levels up to 14,000-fold for viral and 25,000-fold for nonviral transfervectors in nonclonal human cell lines, and up to 2,800-fold in murine hematopoietic cell lines. This improvedregulation was the result of a strong reduction of background expression in the off-state, even if cells weretransduced at high multiplicity of infection, while induction remained at high levels. In addition, the resultsindicated that successful regulation of gene expression in different target cells depended on vector architecture aswell as the choice of the Ptet-promoter.
LAND DER PALMEN UND BLUMEN Blumenriviera – Côte d'Azur Die Côte d'Azur – wie die französische Riviera genannt wird – ist wohl das schönste Stück Erde in Europa. Das azurblaue Meer, die roten und gelben Felsen, die sich im klaren Wasser spiegeln, die subtropischen Pflanzen wie Palmen, Zitronen- und Orangenbäume, das pulsierende Leben in den