Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Using a multi-stakeholder approach to improve governance in pharmaceutical procurement

THE ZAMBIA CASE STUDY REPORT
on Documented Evidence that Civil Society is Influencing
Pharmaceutical Policies and Decisions Relating to Access to
Medicines in SADC Countries.
October 2013
Disclaimer:
This document has been prepared for the UK Department for International Development. Re-Action Consulting (PTY) Ltd. and its
sub-contracted partners in the Responsible Action Consortium accept no responsibility or liability for the consequences of this
document being used in ways that are not responsible or for a purpose other than those for which it was commissioned. Any
agreement, to indemnify Re-Action Consulting and its sub-contracted partners for all loss or damage that might result.
The report should not be relied upon or used for any other project without an independent check being carried out as to its
suitability and the prior written authority of the Responsible Action Consortium.
We accept no responsibility or liability for this document to any party other than the entity by which it was commissioned.
To the extent that this report is based on information supplied by other parties, we accept no liability for any loss or damage
suffered by the client, whether contractual or tortuous, stemming from any conclusions based on data supplied by parties other
than Re-Action Consulting (PTY) Ltd and used by the Responsible Action Consortium sub-contractors in preparing this report.
SARPAM: ZAMBIA CASE STUDY REPORT
Table of Contents
Abbreviations & Acronyms . 4
1. Introduction. 5
2. The Role of Civil Society . 6
3. The TENDAI Project and the CAFs . 7
4. Zambia: Country Background . 10
5. Civil Society Engagement of Policy Makers and Implementers . 11
6. Stories of Impact in Zambia . 13
Story 1: Medicines Stock-outs. 14
Story 2: Health Facility Infrastructure, Stockouts and Human Resources . 16
Story 3: Load Shedding by ZESCO . 18
Story 4: Medicines Supply Chain Management . 20
7. Conclusion . 22
8. Appendix . 23
List of Tendai Project and CAF Co-ordinators . 24
Consumer Action Forum ToRs . 25
Tendai Project Management Dashboard for October 2012 . 28
Zambia Scorecard for March 2013 . 30
Zambia Scorecard for July 2013 . 31
SARPAM: ZAMBIA CASE STUDY REPORT
Abbreviations & Acronyms
Acquired Immune Deficiency Syndrome
Centre for Diseases Control and Prevention
Centre for Infectious Diseases Research in Zambia
Community Officer
Civil Society Organisation
Department for International Development
District Medical Officer
Essential Medicines List
Heavily Indebted Poor Countries
Human Immuno Deficiency Virus
Millennium Challenge Corporation
Memorandum of Understanding
Non-Communicable Disease
Out Patient Department
People Living with HIV and AIDS
Prevention of Mother to Child Transmissions
Southern African Development Community
Southern African Regional Programme on Access to Medicines and Diagnostics
Treatment Advocacy and Literacy Campaign
Tracking Essential National medicines and Diagnostics Access Initiative
United Nations Children's Fund
World Health Organisation
Zambia Electricity Supply Commission
Zambia Health Community Initiative
SARPAM: ZAMBIA CASE STUDY REPORT


1. Introduction
The Southern African Regional Programme on Access to Medicines and Diagnostics (SARPAM), funded by the UK
Department for International Development (DFID), aims to promote a more efficient and competitive market for
essential medicines in order to meet the health needs of poor and underprivileged people in the Southern African
Development Community (SADC).
SARPAM was designed in consultation with Member States, the SADC Secretariat and other stakeholders, to respond
to identified gaps in the pharmaceutical markets of Southern Africa, including market failures, which result in
uncompetitive drug pricing and unreliable availability of medicines.
SARPAM is operating through various programme components known as Partnerships for Action (PACTs) that focus
on Pooled Procurement, Harmonised Regulation, Market Innovations and Investments, Trade and Intellectual
Property Rights, Capacity Building and Technical Support to the SADC Secretariat.
Civil Society seeks to bridge the gap between the SADC leaders and the ordinary citizens
The Civil Society PACT's main focus is to ensure that there is strengthened institutional architecture and partnerships
to improve access to medicines in the SADC region. One of the key outputs of the programme is an increased voice
and influence of civil society reflected in policies on access to medicines and diagnostics in Southern Africa.
Civil Society contributions will add value and supports the purpose and actively participates in pursuit of the
objectives of SARPAM and the principles of the SADC Pharmaceutical Business Plan.
Specifically the Civil Society Pact has also committed itself to ensure that case study reports shall be produced to
demonstrate documented evidence that civil society is influencing pharmaceutical policies and decisions relating to
access to medicines in the Southern Africa Development Community (SADC) countries.
This case study report presents stories that outline the impact that Civil Society has had in Zambia with a focus on
activities undertaken in the last 12 months, from September 2012 to September 2013. The stories outline how
SARPAM: ZAMBIA CASE STUDY REPORT
advocacy work has brought about direct and indirect changes to policies, processes, attitudes and structures that
have in turn improved citizens' access to medicine and healthcare in Malawi.
The stories in this case study tell how community monitors in Zambia are influencing access to medicines at local
facilities through advocacy work as part of the TENDAI project. The stories also speak of the influence advocacy work
has begun to exert in these domains bringing about positive signs for sustainable change and improvement.
Over the past 12 months, this initiative has had tremendous success and this case study report therefore presents
narrative based evidence of the success that Civil Society has had with regard to advocacy thus far in Zambia.
2. The Role of Civil Society
Civil Society Organisations (CSOs) are critical actors in the advancement of universal values around human rights, the
environment, labour standards and anti-corruption. As global development integration has advanced, their role has
gained particular importance in aligning economic activities with social and environmental priorities.
By its very nature, Civil Society plays the role of being the ‘voice of the voiceless', a public watchdog that helps to
highlight the shortcomings of the local government. These organisations are usually able to enter into communities
whose daily hardships often go unnoticed by those in public administration. This then helps the government to keep
track of both the quantity and quality of its performance from a public point of view.
As such, the monitoring of policy implementation and service delivery by the government is a role that Civil Society
always seeks to fulfil with excellence.
Civil Society organisations have been an integral part of SARPAM since its inception. Their local perspectives,
expertise and partnership-building capabilities are indispensable in the evolution and impact of developmental
SARPAM: ZAMBIA CASE STUDY REPORT

African civil society protest at the Abuja+12 meeting in July 2013
In this regard, SARPAM supports Civil Society advocacy initiatives that offer the potential to strengthen the capacity
of regional institutions and civil society to implement joint plans that will achieve agreed results through multi-
stakeholder action across countries in the region. In particular, Civil Society has to date rolled out two major
initiatives that seek to enhance consumer action and interventions in order to help improve access to medicines for
the ordinary majorities in the SADC region.
The first of such initiatives is the TENDAI Project (Tracking Essential National Medicines and Diagnostics Access
Initiative), which utilises a mobile data collection system to monitor community level health care centres by the civil
society members on access to medicines.
The second, and more recent initiative is the establishment of country level Consumer Action Forums (CAFs). The
forums seek to positively influence the pharmaceutical market, including the demand for medicines and their
rational use and advancing access to more affordable medicines.
3. The TENDAI Project and the CAFs
TENDAI, which also means Thank You in Shona, is a civil society initiative under SARPAM that facilitates community-
level collection and use of transparent information about medicines availability, price, quality and resources across
Southern Africa.
It was initiated in 2010 and it partners with local CSOs in participating countries and uses mobile phones to collect
information which is compiled and used as evidence in advocacy campaigns to improve service delivery at those
SARPAM: ZAMBIA CASE STUDY REPORT

Tendai Project Zambia Community Monitors in September 2013
To date the Tendai Project has undergone three different programme phases. The first phase was piloted between
July 2011 and August 2012 and it focused mostly on the local health facility monitoring and mobile based data
collection process.
The second phase was between September 2012 and August 2013. It focused on moving beyond the monitoring and
data collection process and invested in civil society led advocacy interventions.
As from September 2013 the project moved into the third phase that includes a more influential co-ordination role
from the country level Consumer Action Forums (CAFs) as its main focus.
The CAFs seek to positively influence the pharmaceutical market, including the demand for medicines and their
rational use and advancing access to more affordable medicines.
The process of establishing the CAFs is now underway. Towards the end of 2012, SARPAM assisted in the setting up
of the CAFs Malawi, Tanzania, Zambia and Zimbabwe. During 2013 more CAFs have established in additional SADC
countries. It is anticipated that by the end of December 2013, each SADC country will be having a CAF in one level or
SARPAM: ZAMBIA CASE STUDY REPORT

Participants at the CAF Zambia review meeting in Lusaka in September 2013
Crucially, SARPAM has stepped up efforts to formally set up the SADC regional CAF. This process was initiated at a
regional civil society meeting in June 2012. It will culminate with the formal launch meeting at Johannesburg of the
regional CAF in mid-December 2013.
The CAFs are an essential aspect of SARPAM's exit plan and transfer of ownership of civil society advocacy to the
local context. The CAFs, with their intent being sustainability, are expected to be the torchbearers for advocacy
action, promoting scaled-up access to essential medicines beyond SARPAM after December 2014.
SARPAM: ZAMBIA CASE STUDY REPORT

4. Zambia: Country Background
ZAMBIA ECONOMIC INFORMATION
Population:
14,309,466 (2012)
US$23.967 bn (2012)
Per Capita Income:
Gini co-efficient:
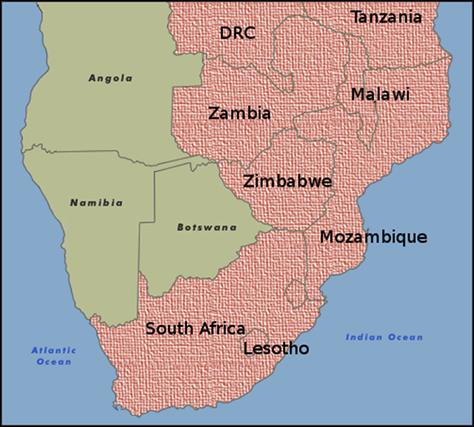
The Republic of Zambia, commonly referred to as Zambia, is a landlocked country located in the Southern part of
Africa and is surrounded by the Democratic Republic of Congo, Tanzania, Malawi, Mozambique, Zimbabwe,
Botswana, Namibia and Angola.
Zambia gained its independence in 1964 from the UK, where Dr Kenneth Kaunda became its first president. From
1972 to 1991, Zambia was a single party state with Kaunda's United National Independent Party as the sole legal
political party. The major political party in Zambia at the moment is The Patriotic Front (PF), led by Michael Sata,
currently president of the country.
Zambia's economy has seen a steady growth over the past seven years.
Nonetheless, poverty remains a significant problem in the country. In 2012, the country's GDP stood at US$23.967
billion and had per capita income of US$1,721. Privatisation of government-owned copper mines in the 1990s
relieved the government from covering mammoth losses generated by the industry.
This increased copper mining output in the country and profitability to spur some economic growth. Copper output
has increased steadily since 2004, due to higher copper prices and foreign investment. In 2005, Zambia qualified for
debt relief under the Highly Indebted Poor Country Initiative, consisting of approximately US$6 billion in debt relief.
As compared to other SADC countries such as Zimbabwe and Malawi, Zambia's economy has seen some marked
SARPAM: ZAMBIA CASE STUDY REPORT
Zambia's dependency on copper makes it vulnerable to depressed commodity prices, but record-high copper prices
and a bumper maize crop in 2010 helped Zambia rebound quickly from the world economic slowdown that began in
2008. Zambia has made some strides to improve the ease of doing business. A high birth rate, relatively high
HIV/AIDS burden, and market distorting agricultural policies have meant that Zambia's economic growth has not
dramatically decreased the stubbornly high poverty rate in the country.
The general state of healthcare in Zambia is poor. Although there are adequate private health facilities in the capital
city, Lusaka, the public health system remains heavily underfunded. Only 50 percent of rural people have access to
health care facilities, often provided by mission hospitals. In comparison, urban dwellers have relatively easier access
Health systems in Zambia are classified into three major categories, where the first level comprising of Health Posts,
Rural Health Centre and District Hospitals, where primary health care and preventive health services are provided.
The second level comprises of the provincial and general hospitals, which provide the curative care and the tertiary
level comprises of Central hospital and the National University teaching Hospital that provide specialized care.
Zambia's health system is currently heavily stretched and only critical injuries or illnesses receive immediate
attention in government hospitals. This could be linked to the fact that Zambian public healthcare is undergoing a
brain drain as a result of doctors leaving the country or preferring to work for higher salaries in the private health
system. There are good private hospitals in Zambia's larger cities, particularly Lusaka. These private hospitals cater
mostly for affluent Zambians and expatriates living in mining communities and compounds owned by organizations
in which they are employed. Similar to other African countries, Zambia has committed to allocate at least 15% of its
national budget on public health care as part of the Abuja declaration agreement. According to The Africa Public
Health Alliance, Zambia has thus far been able to allocate 16.4 %, which puts it slightly above Zimbabwe but yet,
slightly below Malawi.
5. Civil Society Engagement of Policy Makers and Implementers
In Zambia there are two civil society partners that are actively working with SARPAM, which are the Zambia Health
Community Initiative (ZHCI) and the Treatment Advocacy and Literacy Campaign (TALC).
The ZHCI is a national non-governmental organization working with communities to promote a society with healthy
communities. The Initiative was registered in 2009 is currently implementing programs in 9 districts in Zambia and
envisions expanding to 50 more districts by 2015.
SARPAM: ZAMBIA CASE STUDY REPORT
The TALC was formed to lobby for equitable, affordable, and sustainable access to treatment, care, and support for
People Living with HIV and AIDS (PLWHA) in Zambia. The programme seeks to advocate for policy change,
institutional and legal frameworks supporting the access to health care services. In doing so, TALC also seeks to
address issues of HIV/AIDS treatment by making health information easier to access and advocating for community
support. The overall vision of TALC is to create a comprehensive treatment program that is accessible to all and
would lead to a healthy Zambian society free of HIV and AIDS.
The logos for ZHCI and TALC
During September 2012, the ZHCI and TALC with the active support from SARPAM hosted a special training
workshop that sought to enhance the campaign, lobbying and advocacy skills for all community monitors.
The workshop empowered the monitors with skills to continue to actively engage all the relevant authorities and
policy makers on solutions needed to address the identified problems with regards to access to medicines for the
average citizen of Zambia.
Specifically, some key lobbying and advocacy messages for the relevant authorities and policy makers at both district
and national level have also been informed by continual input from the monitors and their respective district
At district level, the monitors have participated at the meetings of the Health Centre Committees (HCCs). During
these meetings, the monitors have been able to highlight the key findings from the monitoring process in a
constructive and engaging way.
The monitors have also been participating at various meetings and events organised by their local district councils.
These include attending the councils' quarterly meetings and also participating in the budget process with particular
focus on health and community access improvement.
The monitors have been using these various meetings and other platforms to highlight some of the issues emerging
from the on-going data collection and monitoring process under the Tendai Project, which have been generally well
received by the relevant stakeholders.
SARPAM: ZAMBIA CASE STUDY REPORT
Some monitors have also been able to set up personal appointments with the local district officials and local
councillors. During these meetings they have managed to highlight the urgency of the need to follow up and act
decisively on all the issues identified during their monitoring work.
6. Stories of Impact in Zambia
This report carries samples of stories of impact based on the advocacy intervention of the community monitors. The
stories presented in this document were gathered at a Monitor's Review meeting held on 5th September 2013. Prior
to the Review Meeting the monitors had received invitations to the session and some story prompting questions
that required them to attend the session with a key story in mind to share. More than 10 stories of impact were
captured. The stories were also referenced against the Tendai InfoHub submissions made by the respective monitors
through the course of the monitoring activities over the last 12 months.
The most significant stories are presented below as a small collection that is indicative of the impact that Civil
Society has had within the Zambian community. Through advocacy, community monitors have been able to address
issues relating to access to medicine within communities. This has then assisted community members with regards
to the free and easily accessible medical treatment.
SARPAM: ZAMBIA CASE STUDY REPORT
Story 1: Medicines Stock-outs
Monitor: Aaron Chiwaala
Area: Lusaka District
Facility: George Clinic
Aaron Chiwaala is a Tendai Monitor from the Lusaka District. He is
an ambitious man and describes himself as "outgoing and
extroverted". He enjoys reading motivational books, taking walks in
nature and spending time writing.
Aaron is assigned to the George Clinic, which is one of the largest
government hospitals in the Lusaka District. It offers primary
healthcare to approximately 150,000 people, of which about 15,
000 are cared for on a daily basis. George Clinic has 68 nurses and
2 doctors on staff.
Aaron grew concerned about a number of issues that were
hindering efficient healthcare services at George Clinic during the
course of 2012 and 2013.
During his monthly monitoring visit he became aware that there were insufficient stock levels of certain medicines at
the Clinic at the beginning of 2013. Essential anti-malaria medicines such as Artemether and Lumefantrine were
frequently unavailable.
Aaron also identified the inconvenience that was caused to patients by a shortage of health personnel, as well as the
discomfort caused by congestion in the clinic's reception area due to insufficient space. One qualified Pharmacy
Technologist at the clinic was required to serve out-patients in two separate departments interchangeably, namely
the Out Patient Department (OPD) and Anti-Retroviral Therapy (ART) section. This shortage of personnel is
ultimately what caused the congestion in the reception area as patients had to stand in long queues for a
considerable amount of time before being attended to.
Aaron's concern was shared by the sister in charge at George Clinic, Mrs Zuze. Together they began to lobby for
improvements to the facility and increased personnel levels. Aaron and Mrs Zuze met with the District Medical
Officer (DMO), Dr Masumba Masaninga, who acknowledged their concerns. After their meeting Dr Masaninga
communicated with the District Medical Stores requesting that they supply anti-malaria medicine in a more timely
and sufficient manner to George Clinic.
SARPAM: ZAMBIA CASE STUDY REPORT
Dr Masaninga wrote a letter to the provincial health officer highlighting the staff shortage that the clinic faced. Dr
Masaninga also notified the Ministry of Health with regards to the need to expand the reception area, with a specific
focus on renovating the OPD and ART sections of the clinic. They requested modifications that would result in having
a more spacious, well-ventilated area. Such modifications would ultimately reduce congestion and noise levels thus
reducing the levels of frustration amongst the awaiting patients.
As a result of the lobbying work carried out by Aaron on conjunction with Mrs Zuze and Dr Masangina, it is apparent
that the requests have brought about improvements at George Clinic. For example, when Aaron performed his
Tendai monitoring on 17th July 2013, George Clinic had the required medicines in stock (please refer to Appendix A).
There is now sufficient stock of Artemether and Lumefantrine 20 and 120mg (Coartem) to meet monthly demands.
The Clinic was also successful in solving the understaffing problem it previously had. As of July of 2013, an additional
Pharmacy Technologist was deployed at George clinic. There are now two Pharmacy Technologists supported by
knowledgeable nurses who have been employed to ease pressure at the ART section of the clinic.
Although the reception area alterations have not come to fruition, Aaron continues to lobby for infrastructure
development at George Clinic. They are yet to be given a response by the Ministry of Health with regard to the plan
of action concerning extending the clinic's reception area.
The George Clinic main entrance
SARPAM: ZAMBIA CASE STUDY REPORT
Story 2: Health Facility Infrastructure, Stockouts and Human Resources
Monitor:
Joseph Fabiano Mvula
Chipata District
Facility:
Joseph Mvula is a Tendai monitor from the Chipata District. He is 43 years of
age and a peer educator and small business owner, in addition to his role as a
monitor. He enjoys recreational activities at local rivers, is an avid reader and is especially passionate about football.
Joseph is assigned to monitoring access to medicines at the
Namusche Clinic, a rural health centre which serves a community of
over 23,000 people. One of the main issues in this area is that there is
a nearby prison that has a high number of HIV positive prisoners who
require treatment. There are more than 260 prisons living with HIV
and AIDS, 40 of which who are on pre ART and another 75 who are on
ART. Current trends are to have all HIV positive patients on ART
regardless of CD4 count. On any given day a healthcare professional
at Namusche could attend to 150 patients.
Through his monitoring activities at the clinic Joseph noticed the need for an Anti Retroviral Therapy (ART) facility, as
the clinic had no facility for people living with HIV/AIDS and TB. Instead, the only available services for such patients
The clinic also experienced stock-outs in relation to HIV/AIDS medicines. These issues prompted Joseph, together
with his team, to approach the ward councillor to request that he take action regarding the conditions at the clinic.
The ward councillor was receptive to their concerns and agreed to take the concerns further. However, when
Joseph was doing his monitoring at Namusche Clinic in March 2013, it came to his attention that there was still a
problem with regard to medicine stocks (refer to Appendix B). Essential medicine such as cotrimoxazole was out of
stock. The only medicines available were four packs of Panado, each pack containing a thousand tablets, six bottles
of 4FDC (4 active ingredients – rifampicin, pyrazinamide, ethambutol, isoniazid – fixed dose combination) containing
672 tablets each and four bottles of Artemether & Lumefantrine, each containing a thousand tablets.
SARPAM: ZAMBIA CASE STUDY REPORT
Inside the Namusche Clinic
The second issue that emerged during Joseph's monitoring was that of a shortage of staff. At that time only 8
healthcare personnel were on duty, while two were on leave. This was causing long queues as each health worker
typically had to attend to an average of 50 patients a day. This was significantly above the required number of
patients to be seen by each health worker.
Joseph organized a meeting with the Health Centre Manager in charge to brief him on his findings. They decided to
meet with the area councillor again and make him aware of the findings. In the meeting they requested the
councillor him to play a more active role in the provision of quality health care and ensure availability of essential
medicines for the benefit of the community members.
Joseph visited Namusche again on 11th October to follow up on the issue he'd raised. The official in charge of the
facility, Mr Tembo, reported that he had also approached the DHO regarding the ART facility. Sadly, the DHO's
response was that they were restricted in terms of the human resources and could not station more healthcare
professionals at Namusche as it is classed as a rural facility and facilities that are classified as rural are not permitted
to have a Doctor, but only a community officer (CO). In addition to the personnel constraint, the DHO highlighted
how there is not enough room at Namusche to house the ART facility they were lobbying for. However, the DHO
informed Mr Tembo that the CIDRZ and CDC were committed to providing assistance in this regard and would visit
soon to commence their services.
SARPAM: ZAMBIA CASE STUDY REPORT
Story 3: Load Shedding by ZESCO
Monitor:
Facility:
Linda Healthcare Facility
Location:
Livingstone District
Lloyd Bwalya is a Tendai monitor based in the Livingstone District who is married
and has five children. Lloyd studied prosecution, law and political studies at college.
He worked for Zambia Railways from 1989 to 2001, but was retrenched. He now
works as a volunteer with NZP as a co-ordinator.
Linda Healthcare facility is a rural health centre, which provides services to approximately 11,000 people from three
communities. The facility serves approximately 55 patients a day and is staffed
by 18 nurses. Since 2006, the Southern Province Minister, Alice Simango, has
had a facelift including the building of male and female wards.
Electricity load shedding in recent times has however hampered the facility. The
blackouts have caused serious disruptions at the facility. For example, night
shift staff have particular difficulty in carrying out their duties during a blackout
as they are reliant on candles and are not able to attend to the patients as well
as they should. The blackouts have been so severe that some patients had to be
transported to the nearby Maramba Clinic for care. The clinic has also had to
turn away some patients, as they could not be attended to.
In pursuit to resolve this issue, Lloyd organised a meeting between Linda Healthcare representatives, the District
Commissioner, the District HIV/AIDS Coordinating Advisor and the District HIV/AIDS Task Force Team and some
representatives from the local electricity supplier, ZESCO. The meeting was held on the 4th of June 2013 and the aim
was to reach agreement on a solution to the electricity blackout problem.
The outcome of the meeting was that a letter should be written to senior ZESCO management requesting them to
connect the Clinic to a non-load shedding power line. The copies of the same letter were sent to the Member of
Parliament, District commissioner, District Medical officer, the District Coordinating advisor, NZP district
Chairperson, District HIV /AIDS task force chairman and the sister-in-charge at Linda Healthcare Facility.
As a result of the meeting held on the 4th of June, the monitors managed to secure another a meeting with the
ZESCO, including management, to discuss the possibility of connecting Linda clinic to a non-load shedding line. In
that meeting ZESCO management agreed to conduct a survey for possible re-connection within two weeks, to
SARPAM: ZAMBIA CASE STUDY REPORT
respond in writing to share the findings of the survey and recommendations and then implement the
recommendations of the survey report.
Outside the Linda Clinic
As of today, ZESCO have installed the necessary pole infrastructure at the facility but are yet to connect the clinic to
the new non load shedding line. Lloyd reports that the area councillor has been in contact with ZESCO, as recently as
29th,October to push for feedback and they have promised to give an indication of when the line will be connected
by the end of October 2013.
SARPAM: ZAMBIA CASE STUDY REPORT
Story 4: Medicines Supply Chain Management
Monitor:
Luanshya District
Facility:
Ronald Mpande is a Tendai monitor in the Luanshya District of Zambia. Ronald
is married with three children and is an electrician by profession.
Ronald is assigned to Chibolya Clinic. The clinic is classified as an urban facility
and is located within the city of Luanshya. Chibolya serves a population of
approximately 19,983 people with a staff compliment of 15 nurses.
One of the significant issues Ronald's monitoring highlighted was how, in terms of
the local supply chain management of medicines at public facilities, the health
facilities in Luanshya District were only allowed to order medicine once a month
from the central stores.
As a result, ordering medicines once a month caused unnecessary shortages of
essential medicines at Chibolya Clinic as the medicine stock tended to finish prior to
the next ordering date. On 18th May 2013, Ronald took the initiative to organise a
meeting that aimed to resolve the prevailing system of ordering medicine from the
district pharmacy. Present in the meeting was the Luanshya team and the District
Medical Officer.
After much deliberation, the meeting concluded that the District Medical Officer would write a letter to the
Provincial Health Office. In the letter, he would request that they allow his office to order medicines twice a month
to avoid medicine stock-outs. This meeting also birthed a follow up meeting, which was then held on the 30th June
2013. The meeting took place at the DMO's office and present in the meeting were pharmacists from various clinics
and hospitals, nurses in charge and a councillor from Luanshya municipal council.
SARPAM: ZAMBIA CASE STUDY REPORT
Inside the Chibolya Clinic and the Local Catchment Area Map
Ronald is pleased to advise that the meetings were successful. In the end, the DMO received permission to allow
Luanshya facilities to order medicines on a bi-monthly basis from the district pharmacy.
SARPAM: ZAMBIA CASE STUDY REPORT
7. Conclusion
Zambia has showed a steady growth in its economy, and even though its GDP is slightly better as compared to some
SADC countries, its public health system remains heavily underfunded. As poverty still prevails within the country,
Civil Society has played a significant role in influencing the access of medicine within communities in Zambia. Since
the end of 2012 and through-out the current year (2013), the advocacy and lobbying undertaken by the community
monitors has brought forth hope to the average Zambian communities. The monitors have been able to confront
challenges regarding the availability and access of medicine to all. Their efforts have seen that in some instances,
changes in practice are enforced to ensure efficiency in health care facilities.
Civil society lobbying has achieved sufficient stock levels of Artemether and Lumefantrine 20 and 120mg (Coartem)
meeting the supply demands at Namusche clinic in Chipota district. Another success story reported by Joseph who
monitors is bringing to the attention of authorities the ill effects of staff shortages in healthcare facilities. Although
some problems remain unresolved civil society sustain the pressure to authorities and ensure that the highlighted
issues receive constant attention.
The monitors also have been able to follow up on matters such as understaffed health care facilities, medicine stock-
outs, and infrastructure-related concerns. In some cases, solutions were adopted addressing such challenges,
whereas in other instances, the monitors have taken initiatives that would then lead to the changing or
improvement of the status quo in the near future.
The impact stories have been selected as samples representing several other emerging impact stories that have been
considered for this year's report. Some of the emerging stories will be fully considered for the 2014 report.
These selected sample stories do to a large extent show evidence that under the Tendai Project, the Civil Society as
co-ordinated by the ZHCI and TALC campaign has already started to successfully engage and influence the
pharmaceutical policies and decisions relating to access to medicine in Zambia. This positive trend is set to continue
during the next year, as the civil society advocacy efforts will start to expand from the community level to the
national level. This will be enabled by the process of linking up the efforts of the monitors with the broader national
level civil society advocacy strategy on promoting access to medicines as co-ordinated by the organisations working
under the CAF in Zambia.
It is hoped that by December 2014, more documented evidence will have emerged proving so much as to how the
Civil Society in the country is successfully improving access to medicines for the average citizens in the country by
actively engaging all the relevant authorities and policy makers under the auspices of the Tendai Project.
SARPAM: ZAMBIA CASE STUDY REPORT
8. Appendix
Letter of Authority for the Tendai Project
SARPAM: ZAMBIA CASE STUDY REPORT
List of Tendai Project and CAF Co-ordinators
Please find below the list of the country level Co-ordinators for both the Tendai Project and the CAFs:
1. Angola – Simao Cacumba M Faria, [email protected] , SCARJoV
2. Botswana – Una Ngweny Botswana Family Welfare Association (BOFWA)
3. DRC – Mike Upio, [email protected], Centre for Medical Evangelism (CME)
4. Lesotho – Shale Sofonea, [email protected] , Development for Peace Education, (DPE)
5. Malawi – Sam Jeke, Global Hope Mobilisation, (GLOHOMO). For the CAF – Caleb Thole,
Global Hope Mobilisation, (GLOHOMO).
6. Mauritius – Vidya Charan, [email protected], Mauritius Family Planning and Welfare Association
7. Mozambique – Cesar Mufanequico, Mozambique Treatment Access Movement
(MATRAM). For the CAF, Sally Griffin from NAIMA
8. Namibia – Corinna van Wyk,, Legal Assistance Centre, (LAC). For the CAF, Sandi Tjaronda,
Namibian Network of AIDS Service Organisations (NANASO),
9. Seychelles – Justin Fremont, [email protected] HIV and AIDS Support Organisation (HASO)
10. South Africa – Kerry Cullinan, Health-E
11. Swaziland – Siphiwe Hloph, Swaziland Positive Living, (SWAPOL)
12. Tanzania – Phillip Nyakanyenge, [email protected], Pamoja Tupambane wa Tanzania, (PATUTA). For the
CAF, Chris Awinia, [email protected] , PRAXIS Tanzania
13. Zambia – Casco Mubanga, [email protected], Zambia Health Community Initiative, (ZHCI). For the CAF,
Banza Chela, [email protected] , Treatment Advocacy and Literacy Campaign, (TALC)
14. Zimbabwe – Faith Kowo, [email protected] , Community Working Group on Health, (CWGH)
SARPAM: ZAMBIA CASE STUDY REPORT
Consumer Action Forum ToRs
SARPAM Civil Society PACT
Terms of Reference for the Consumer Action Forums
The Southern Africa Regional Programme on Access to Medicines and Diagnostics (SARPAM) Civil Society
(CS) Pact; with the active support of the Department for International Development (DFID), hosted the
inaugural regional Consumer Action Forum (CAF) meeting in Johannesburg on Tuesday 19th June 2012.
This was the first major face to face meeting of the civil society network on access to medicines in the
Southern Africa Development Community (SADC) region since the end of the inception phase of SARPAM in
January 2010. As such, the meeting provided a good platform to review the role of civil society in efforts to
improving access to medicines in the SADC region.
The objective of the meeting was to promote consumer and civil society perspectives on scaling up and
sustaining improved access to medicines in the SADC region
One of the key resolutions of the June 2012 meeting was to identify and create a database of civil society
organisations that are actively interested in scaling up consumer action on improving access to medicines,
and set up country level Consumer Action Forums (CAFs)
Role of the Consumer Action Forums
a) There shall be CAFs at a country level that shall be set up by CS that shall seek to positively influence
the pharmaceutical market including the demand for medicines and their rational use and advancing access to more affordable medicines.
b) The CAFs shall develop a media and advocacy programme of action to raise public awareness of all
efforts aimed at scaling up consumer action on improving access to medicines at national and regional levels.
c) The CAFs shall develop a resource mobilisation strategy to fund efforts of the CS to scale up consumer
action on improving access to medicines considering all available options including national budgets, Abuja Declaration, Financial Transaction Tax and other various international funding facilities.
d) The CAFs shall assist the collation of evidence that civil society is influencing pharmaceutical policies and
decisions relating to access to medicines in SADC in line with the targets set under the Pharmaceutical Business Plan.
SARPAM: ZAMBIA CASE STUDY REPORT
Membership of the CAFs
a) Membership of the CAFs shall only consist of institutional CS organisations that are actively interested in
the promotion of access to medicines in that country.
b) For the avoidance of doubt, the CAFs shall not have any form of individual membership
c) The CAFs shall consist of no less than five institutional members at any given time; and where the
membership is less than five, operations of that CAF shall be suspended temporarily until the minimal quota is met again.
d) The membership of the CAFs shall be confirmed by way of a signed registration form
e) The membership data base of the CAFs shall be kept by the Co-ordination Committees
f) The CAFs shall hold at least one general meeting every year.
Role of the CAFs Co-ordination Committees
a) There shall be a Co-ordination Committee (CC) that shall facilitate the day to day administration and
representation of the CAFs in between general meetings.
b) The CCs members shall be nominated in a representative capacity of their own organisation and never in
an individual capacity.
c) The CCs shall be constituted of at least four institutional members at any given time; and where the
number is less than four members, co-options shall be allowed.
d) During their initial meeting, the four representatives shall elect among themselves, a Chairperson, Vice
Chairperson, Secretary and a Treasurer
e) Resources permitting, the CCs shall appoint a Co-ordinator who shall act as the secretariat as ex-officio
members of the Committee.
Tenure of the Co-ordination Committees
a) All the CCs members shall serve for a one two- year term or but shall be eligible to offer themselves for
re-election for one more term.
b) Any CCs member may cease to hold office if he/she ceases to hold such an office or post enabling
him/her to be a member; the other CCs members endorse his/her written resignation to the Chairperson or if he/she abstains from two consecutive meetings without any reasonable excuse or is unable to continue being a member of the CCs for any other reason.
SARPAM: ZAMBIA CASE STUDY REPORT
c) In the event of a member abstaining from any CC meeting for two consecutive occasions, the CCs
Chairperson shall write to the member concerned as well as the organisation seeking for an explanation. If there is no response to the communication within a period of two weeks or if the explanation is deemed by the majority of CCs members to be unsatisfactory, then a vacancy will be declared.
d) In the event that a vacant post arises in the CCs, the relevant organisation shall nominate a replacement
or where not possible, the CCs shall instead co-opt a person of their own choice by consensus.
e) Any person who may be co-opted into the CCs should also meet the requirements of being a CCs
member and shall serve for the remainder of the period not served by the member vacating.
f) A member so co-opted will be eligible for re-election if serving on a first term.
Authority and Duties of the Co-ordination Committees
a) In between the general meetings of the CAFs, the CCs shall be the highest referral body on any issues
pertaining to the implementation process of the CAFs in line with Section 4 (a).
b) The CCs shall also represent the CAFs in any events, meetings or committees that are related to the
implementation process of the CAFs.
c) The CCs shall in general provide advice and offer guidance and moral support to both the Co-ordinator
and any other secretariat members of the CAFs.
Meetings of the Co-ordination Committees
a) The CCs shall have regular meetings that shall be convened by the Chairperson, to discuss all relevant
matters related to the CAFs.
b) The CCs meetings shall be held at least once every three months, preferably in February, May, August
c) The Chairperson may convene and preside over any additional meeting(s) of the CCs, if circumstances
deem one necessary.
d) The meetings shall have a quorum of no less than two members excluding the Co-ordinator.
e) The resolutions of the meetings shall as much as possible be based on consensus but where necessary,
shall have to be endorsed by at least two-thirds majority of all the members.
f) The Co-ordinator shall act as the Minutes Secretary of all the CCs meetings
SARPAM: ZAMBIA CASE STUDY REPORT
Tendai Project Management Dashboard for October 2012
SARPAM: ZAMBIA CASE STUDY REPORT
SARPAM: ZAMBIA CASE STUDY REPORT
Zambia Scorecard for March 2013
SARPAM: ZAMBIA CASE STUDY REPORT
Zambia Scorecard for July 2013
SARPAM: ZAMBIA CASE STUDY REPORT
Source: http://narrativelab.co.za/wp-content/uploads/2014/04/CSR-Zam-1Nov13.pdf
BIM Implementation: An Owner's Guide to Getting Started CURT Owner Member Companies Abbott Laboratories Air Products & Chemicals, Inc. The Procter & Gamble Company Alstom Power, Inc. Salt River Project Shell Global Solutions (U.S.), Inc. American Electric Power Southern Companies Barrick Gold Corporation Baxter Healthcare Corporation
La corrosion humide Sauf indication contraire, les potentiels sont mesurés par rapport à une électrode standard à hydrogène. 1. Présentation des phénomènes 1.1. Généralités La corrosion est le phénomène par lequel les métaux et les alliages subissent de la part de leur environnement une oxydation en ions métalliques, éventuellement complexés par le milieu.