Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
Scure.co.kr
CLINICAL TRIALS AND OBSERVATIONS
Local tumor invasiveness is more predictive of survival than InternationalPrognostic Index in stage IE/IIE extranodal NK/T-cell lymphoma, nasal typeTae Min Kim, Yeon Hee Park, Sang-Yoon Lee, Ji-Hoon Kim, Dong-Wan Kim, Seock-Ah Im, Tae-You Kim, Chul Woo Kim,Dae Seog Heo, Yung-Jue Bang, Kee-Hyun Chang, and Noe Kyeong Kim
This study was launched to determine the
was observed in 23 patients. Using multi-
nificant factor for reduced DFS. Ann Ar-
prognostic significance of local tumor
variate analysis, factors associated with
bor staging system did not predict CR,
invasiveness (LTI) in 114 patients diag-
low probability of CR were the presence
OS, or DFS but IPI did have predictive
nosed with stage IE/IIE extranodal natural
of LTI (P < .001), the presence of B symp-
power with regard to survival outcome.
killer (NK)/T-cell lymphoma, nasal type
toms (P ⴝ
.003), and single-modality che-
LTI is the most important prognostic fac-
(NTCL). LTI was defined as bony invasion
motherapy (P ⴝ
.045). The presence of
tor in predicting low probability of CR and
or destruction or tumor invasion of the
LTI (relative risk [RR] ⴝ
8.4, 95% confi-
reduced OS and DFS in nasal stage IE/IIE
skin. Complete remission (CR), overall
dence interval [CI] 3.9-17.9; P < .001) and
NTCL. (Blood. 2005;106:3785-3790)
survival (OS), and disease-free survival
high IPI score (RR ⴝ
2.8, 95% CI 1.2-6.8;
(DFS) were compared between each group
P ⴝ
.019) were also predictive of OS. The
according to LTI, Ann Arbor stage, and
presence of LTI (RR ⴝ
7.3, 95% CI 3.2-
International Prognostic Index (IPI). LTI
16.5; P < .001) was an independently sig-
2005 by The American Society of Hematology
The Ann Arbor staging classification system was originally devel-
patients of nasal stage IE/IIE NTCL.13 However, the Ann Arbor
oped for Hodgkin lymphoma, but in the absence of a better
stage failed to predict survival differences between stage IE and
alternative it has also been used for staging non-Hodgkin lympho-
stage IIE in the Korean multicenter study.13 It also posed clinical
mas (NHLs) for over 30 years.1 However, in some studies the Ann
challenges in treatment selection due to its inability to predict the
Arbor classification fails to identify the more aggressive prognostic
heterogeneous clinical behaviors of nasal stage IE/IIE NTCL, which
subgroups of NHLs2,3 that spread to discontiguous lymph nodes
included paranasal extension, bone destruction, and skin involve-
and extranodal sites. For a more accurately systematized prediction
ment.6,14-16 The extent of nasal lymphoma was considered as a
of survival outcome, the International Prognostic Index (IPI) had
prognostic factor in a few studies.17,18 Therefore, we aimed to
been developed for aggressive B-cell lymphoma4 and has also been
compare the prognostic accuracies of a system based on local
applied to T-cell lymphoma.5
tumor invasiveness (LTI) with the existing Ann Arbor stage and the
The extranodal natural killer (NK)/T-cell lymphoma, nasal type
IPI, which has been shown to correlate with survival in recentstudies in nasal stage I
(NTCL), is a distinct clinicopathologic entity that is very rare in
Western populations but rather common among Asians, Mexicans,and South Americans of American Indian descent.6-8 A recentnationwide study of malignant lymphomas in Korea revealed that
Patients, materials, and methods
NTCL accounted for 8.7% to 10.5% of all NHLs and 74.1% oflymphomas arising in the nasal cavity and paranasal sinuses.9,10
Clinically, it often destroys the facial midline and spreads to or
We screened all 179 patients newly diagnosed with NTCL at Seoul National
relapses at extranodal sites. Pathologically, it has a broad cytologic
University Hospital (n ⫽ 134) and Korea Cancer Center Hospital (n ⫽ 45)
spectrum varying from pleomorphic mixed, small, medium, or
in Seoul, Korea, between July 1991 and October 2003. Sixty-five cases
large cells to predominantly large cells. The tumor cells are
were excluded in the analysis for the following reasons: 40 patients hadextranasal NTCL, 16 patients had nasal stage III
characteristically positive for CD56, CD2, cytoplasmic CD3 (CD3⑀),
E/IVE NTCL, 1 patient was
lost to follow-up, 1 patient had blastic NK cell lymphoma, and 7 patients
and CD45R0 by immunophenotyping and positive for Epstein-Barr
received no treatment. A total of 114 patients with typical histologic
virus (EBV) by in situ hybridization.6,11,12 Patients who presented
features of NTCL,6 primary tumors localized to the upper aerodigestive
with nasal stage IIIE/IVE and extranasal NTCL exhibited more
tract, and Ann Arbor stage IE/IIE were included in a retrospective
aggressive tumor behavior and poorer prognosis compared with
intent-to-treat analysis. All patients had undergone a staging work-up
From the Department of Internal Medicine, Seoul National University Hospital,
Welfare, Republic of Korea (0412-CR01-0704-0001).
Cancer Research Institute, Seoul National University College of Medicine,
Reprints: Dae Seog Heo, Department of Internal Medicine, Seoul National
Seoul, Korea; Department of Internal Medicine, Korea Cancer Center Hospital,
University Hospital, 28 Yongon-dong, Chongno-gu, Seoul, 110-744, Korea; e-
Seoul, Korea; and Departments of Radiology and Pathology, Seoul National
University College of Medicine, Seoul, Korea.
The publication costs of this article were defrayed in part by page charge
Submitted May 23, 2005; accepted August 4, 2005. Prepublished online as
payment. Therefore, and solely to indicate this fact, this article is hereby
Blood First Edition Paper, August 18, 2005; DOI 10.1182/blood-2005-05-2056.
marked ‘‘advertisement'' in accordance with 18 U.S.C. section 1734.
Supported by a grant of the Korea Health 21 R&D Project, Ministry of Health &
2005 by The American Society of Hematology
BLOOD, 1 DECEMBER 2005
䡠 VOLUME 106, NUMBER 12
BLOOD, 1 DECEMBER 2005 䡠 VOLUME 106, NUMBER 12
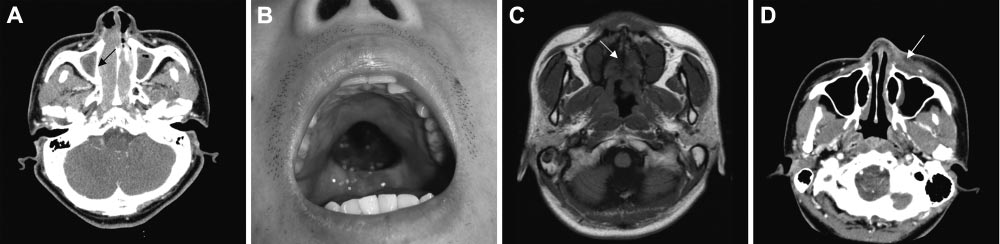
Figure 1. Local tumor invasiveness. (A) Thinning of right medial wall of maxillary bone (arrow) in CT of paranasal sinuses. (B) Palatal perforation on physical examination. (C)
High signal intensity of hard palate is not delineated in T1-weighted MRI (arrow). (D) Skin infiltration by tumor (arrow) in CT of paranasal sinuses. Picture was taken with an
Olympus Camedia C4000Z camera (Olympus, Tokyo, Japan). Adobe Photoshop 6.0 was used to process images (Adobe, San Jose, CA).
including panendoscopy of the upper aerodigestive tract, chest radiograph,
mycin, and procarbazine; 15 patients), ProMACE-CytaBOM (cytarabine,
computed tomography (CT)/magnetic resonance imaging (MRI) of the
bleomycin, vincristine, methotrexate, leucovorin, prednisolone, doxorubi-
head and neck, CT of the abdomen and pelvis, and bone marrow
cin, cyclophosphamide, and etoposide; 1 patient), EPOCH (etoposide,
examination. Contiguous disease extending to adjacent structures was
prednisolone, vincristine, cyclophosphamide, and doxorubicin; 3 patients),
staged as IE and lymph nodes that are 1.5 cm or greater were considered to
and IMVP-16 (ifosfamide, methotrexate, etoposide, and prednisolone; 15
be abnormal. Response to treatment was assessed according to the response
patients). The total radiation dose ranged from 25.2 Gy to 64.8 Gy (mean
criteria for NHLs.20 This study was approved by the institutional review
dose, 47.0 Gy).
board at the Seoul National University Hospital. Informed consent wasprovided according to the Declaration of Helsinki.
Local tumor invasiveness
The association between clinical factors and the probability of attainingcomplete remission (CR) was evaluated by the Pearson 2 test. Overall
LTI was defined as bony invasion or perforation or invasion of the skin. The
survival (OS) was measured from the date of diagnosis to the date of death
involved bony structures included the anterior and medial walls ofmaxillary sinuses; the medial walls of the orbit; the anterior and inferiorwalls of ethmoidal sinuses; the skull base; and the inferior walls of frontal
Table 1. Characteristics of 114 nasal stage IE/IIE extranodal NK/T-cell
sinuses, hard palate, nasal bone, and nasal septal bones (perpendicular plate
of ethmoid and vomer). We defined the extent of bone involvements based
No. of patients (%)
on CT and physical findings. Thinning or disorganized structure of bonesdue to the tumor was regarded as bony invasion (Figure 1A), and bone
Age, n ⴝ 114
defect caused by the tumor was regarded as bony perforation (Figure 1B).
60 y old or younger
Disruption of high signal intensity of bone marrow on T1-weighted MRI
was also considered as bony invasion (Figure 1C). The infiltration of
Sex, n ⴝ 114
overlying skin around the tumor was regarded as skin invasion (Figure 1D).
The CT/MRI findings of the head and neck were reviewed by radiologists
(J.-H.K. and K.-H.C.) blinded to clinical outcomes.
Primary sites of tumor, n ⴝ 114
Histology, immunophenotyping, and detection of EBV
Oral cavity/oropharynx
All pathologic specimens were reviewed and reclassified based on strict
morphologic criteria in adjunction with immunophenotypic analyses6 by a
Systemic symptoms, n ⴝ 113
single pathologist (C.W.K.). Immunophenotypic procedures were per-
formed on paraffin sections using a routine avidin-biotin–peroxidase
complex method by using the following antibodies: CD3⑀ (DakoCytoma-
Performance status, n ⴝ 114
tion, Copenhagen, Denmark), CD20 (DakoCytomation), CD45R0 (DakoCy-
tomation), and CD56 (Monosan, Uden, The Netherlands; DiNonA, Seoul,
Korea). EBV RNA in situ hybridization (ISH) was performed using an ISH
Ann Arbor stage, n ⴝ 114
detection kit (Novocastra, Newcastle upon Tyne, United Kingdom).
Histologic findings showed angiocentricity (86% of patients), necrosis
(98%), and pleomorphic infiltration (89%). Immunophenotypes were
LDH level, n ⴝ 109
CD56⫹CD3⑀⫹CD20⫺ (92 patients), CD56⫺CD3⑀⫹CD20⫺ (12 patients),
and CD56⫹CD3⑀⫺CD20⫺ (2 patients). Sixty-one (98%) of 62 patients
expressed CD45R0. Forty-six (75%) of 61 patients harbored EBV RNA.
No. of extranodal sites, n ⴝ 114
International Prognostic Index rating, n ⴝ 112
Treatment modalities were given as follows: combination treatment of 3 to
6 cycles of chemotherapy with involved-field radiation therapy (56
patients), chemotherapy alone (45 patients), or radiation therapy alone (13
Immunophenotyping, n ⴝ 106
patients). Selection of treatment modality was at the discretion of the
treating physicians. The chemotherapy regimens included CHOP (cyclophos-
phamide, doxorubicin, vincristine, and prednisolone; 67 patients), COP-
BLAM-V (cyclophosphamide, doxorubicin, vincristine, prednisolone, bleo-
BLOOD, 1 DECEMBER 2005
LOCAL TUMOR INVASIVENESS IN NK/T-CELL LYMPHOMA
䡠 VOLUME 106, NUMBER 12
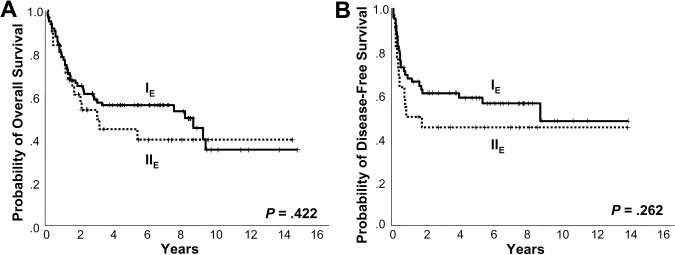
Figure 2. Kaplan-Meier plots of Ann Arbor stage.
Kaplan-Meier plots of (A) overall survival and (B) disease-
free survival according to Ann Arbor stage.
or the last follow-up visit. For patients in CR, disease-free survival (DFS)
pendently significant factors were the presence of LTI (RR ⫽ 16.0,
was calculated from the date of CR to the first evidence of relapse. OS and
95% CI 4.2-61.5; P ⬍ .001), the presence of B symptoms
DFS curves were derived by the Kaplan and Meier method.21 Univariate
(RR ⫽ 7.4, 95% CI 2.0-27.3; P ⫽ .003), and chemotherapy alone
analysis of OS or DFS was performed using the log-rank test. Factors
(RR ⫽ 3.6, 95% CI 1.0-12.9; P ⫽ .045). EBV RNA positivity did
independently associated with OS or DFS were identified by multivariateanalysis using the Cox proportional hazards regression model.22 Two-sided
not adversely affect the attainment of CR (P ⫽ .125).
P values of less than .05 were considered significant. All statistical analyses
were performed using SPSS version 11.0 (SPSS, Chicago, IL).
The 5-year OS and DFS were 53% and 55%, respectively. At thetime of analysis, 56 patients were alive and 58 had died due to the
lymphoma itself (n ⫽ 44), treatment-related complication (n ⫽ 8),and other comorbid disease (n ⫽ 6). Positive EBV RNA showed a
Patients and treatment outcomes
trend of negative correlation with OS and DFS (5-year OS 46% vs
The clinical characteristics of the 114 patients are summarized in
63%, P ⫽ .125; 3-year DFS 46% vs 69%, P ⫽ .099). Ann Arbor
Table 1. Median age of our sample was 47 years with a male-female
stage IE did not show better 5-year OS and DFS compared with Ann
ratio of 1.7:1. Median follow-up period for survivors was 78
Arbor stage IIE (5-year OS 56% vs 44%, P ⫽ .422; 5-year DFS
months (range, 17-177 months). One third of the patients presented
59% vs 45%, P ⫽ .262; Figure 2A-B). However, the OS and DFS
with systemic symptoms, most of whom had an ambulatory
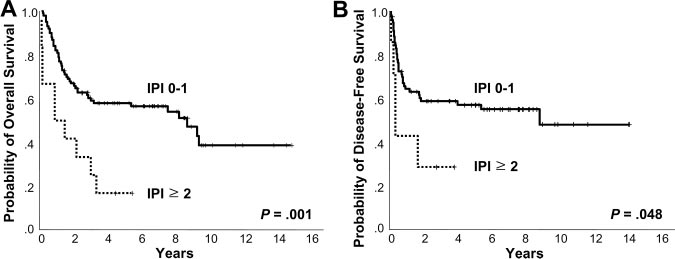
were superior in the low IPI score subgroup (0-1) compared with
performance status (PS; Eastern Cooperative Oncology Group
the high IPI score (ⱖ 2) group (5-year OS 58% vs 17%, P ⫽ .001;
[ECOG] 0-1). Nearly three fourths of patients showed Ann Arbor
3-year DFS 59% vs 29%, P ⫽ .048; Figure 3A-B). The presence of
stage IE, and elevated lactic dehydrogenase (LDH) level was
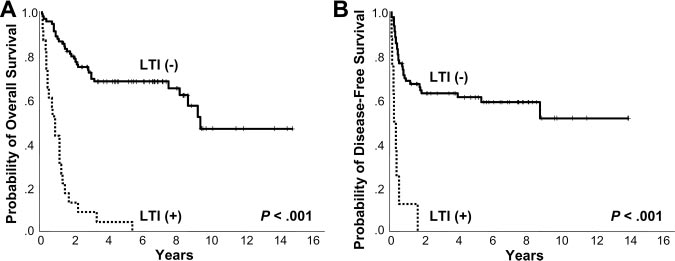
LTI reduced OS and DFS (5-year OS 4% vs 68%, P ⬍ .001; 1-year
observed in one third of the patients. One hundred (89%) of 112
DFS 13% vs 68%, P ⬍ .001; Figure 4A-B). In terms of treatment
patients were classified as having low IPI scores (0-1) and only 1
modality, there were no significant differences in OS and DFS
patient had bulky disease. Forty-six (82%) of 56 patients treated
between the combined modality, radiation alone, and chemo-
with combined modality achieved CR, but 16 (35%) of the 46
therapy alone groups (5-year OS 56%, 69%, and 44%, respectively,
patients in CR eventually relapsed. CR was achieved in 28 (62%)
P ⫽ .191; 5-year DFS 66%, 55%, and 39%, respectively, P ⫽ .087).
of 45 patients receiving chemotherapy alone, of whom 17 (61%)
In addition, chemotherapy regimens did not influence treatment
subsequently relapsed. In the radiation alone group, 11 (85%) of 13
outcome (data not shown).
attained CR but 6 (55%) of 11 relapsed.
Using univariate analysis, the factors associated with lower
Prediction of survival
probability of achieving CR were the presence of LTI (relative risk[RR] ⫽ 15.0, 95% confidence interval [CI] 4.9-45.4; P ⬍ .001),
The clinical factors associated with reduced OS in univariate
ECOG PS of 2 or higher (RR ⫽ 7.5, 95% CI 1.3-43.9; P ⫽ .025),
analysis were the presence of LTI (RR ⫽ 8.5, 95% CI 4.7-15.2;
the presence of B symptoms (RR ⫽ 4.9, 95% CI 1.9-12.5;
P ⬍ .001), high IPI score (RR ⫽ 3.0, 95% CI 1.5-6.0; P ⫽ .002),
P ⫽ .001), and chemotherapy alone (RR ⫽ 3.3, 95% CI 1.3-8.1;
number of extranodal sites (no. ENSs) of 2 or more (RR ⫽ 2.7,
P ⫽ .011). In a subsequent multivariate regression analysis, inde-
95% CI 1.3-5.6; P ⫽ .006), and advanced age (⬎ 60 years;
Figure 3. Kaplan-Meier plots of IPI. Kaplan-Meier plots
of (A) overall survival and (B) disease-free survival
according to International Prognostic Index.
BLOOD, 1 DECEMBER 2005 䡠 VOLUME 106, NUMBER 12
Figure 4. Kaplan-Meier plots of LTI. Kaplan-Meier plots
of (A) overall survival and (B) disease-free survival
according to local tumor invasiveness.
RR ⫽ 1.8, 95% CI 1.0-3.4; P ⫽ .047; Table 2). Using multivariateanalysis, independently significant factors were the presence of LTI
(RR ⫽ 8.4, 95% CI 3.9-17.9; P ⬍ .001) and high IPI score(RR ⫽ 2.8, 95% CI 1.2-6.8; P ⫽ .019; Table 3). The presence of
The data presented here indicate that the presence of LTI provides
LTI and high IPI score remained independently significant in
the highest RR for reduced OS and DFS and low probability for CR
treatment modality–stratified multivariate analysis.
in patients with nasal stage IE/IIE NTCL compared with other
In terms of DFS, the factors associated with reduced survival
clinical factors. Although high IPI score was predictive of reduced
were the presence of LTI (RR ⫽ 7.0, 95% CI 3.1-16.0; P ⬍ .001),
OS, the IPI score itself did not predict CR and DFS in multivariate
no. ENSs of 2 or more (RR ⫽ 2.9, 95% CI 1.0-8.2; P ⫽ .045),
analysis. Ann Arbor stage was unable to dissect prognostic
and elevated LDH level (RR ⫽ 1.9, 95% CI 1.0-3.7; P ⫽ .047)
subgroups in our analysis.
by univariate analysis. High IPI score showed trend of nega-
Robbins et al17 previously reported that 5-year DFS was
tively affecting DFS (RR ⫽ 2.5, 95% CI 1.0-6.5; P ⫽ .057). The
shortened in advanced T stages using the tumor-node-metastasis
presence of LTI was an independently significant factor for
(TNM) staging system in stage IE/IIE lymphomas of nasal cavity
reduced DFS (RR ⫽ 7.2, 95% CI 3.2-16.5; P ⬍ .001) using
and paranasal sinuses. Similarly, Logsdon et al18 reclassified stage
multivariate analysis. By treatment modality–stratified analy-
IE into T stages according to the extent of the disease and showed
sis, the presence of LTI and advanced age were significantly
that early T stages improved freedom from progression in patients
associated with reduced DFS. However, Ann Arbor stage did
treated with radiation therapy. Despite lack of immunophenotyp-
not affect OS and DFS in univariate analysis (P ⫽ .423 and
ing, the 2 studies used the TNM staging system and focused on the
extent of the lymphoma, including bone destruction.18 The majorityof studies to date showed the local invasive nature of nasal
Local tumor invasiveness
lymphomas extending to adjacent anatomic structures14,17,18,23,24and destroying bone structures.6,16,25 Paranasal extension was a
Twenty-three (21%) of 111 patients presented with LTI and
significant predictive factor of survival in several studies,17,18,26,27
characteristics are shown in Table 4. The median duration of
whereas Cheung et al28 reported no prognostic significance of
presenting symptoms was 4 months (range, 1-13 months). The
paranasal extension or the significance of bony invasion. Here, we
patterns of failure were as follows: local, 15 patients; regional, 2
investigated LTI that indicated a more advanced disease state than
patients; and systemic, 15 patients. The sites of systemic failure
paranasal extension. With the presence of LTI, the majority of
were gastrointestinal tract, lung, skin, bone marrow, liver, testis,
patients with systemic failure had the predilection sites of skin,
and central nervous system (CNS). Eight (36%) of 22 evaluable
gastrointestinal tract, liver, testis, and CNS, consistent with previ-
patients attained CR but relapsed early (median DFS 3.0
ous findings.29,30 Relative high frequency of systemic failure (65%)
months). All patients died of lymphoma (n ⫽ 20) or treatment-
in patients with LTI resulted in reduced survival duration. Further-
related complications (n ⫽ 3), and median OS was 10.6 months.
more, systemic failure was not prevented by conventional treat-
Treatment modality significantly affected median OS (combined
ments and led to death after the occurrence. Although combined
modality vs chemotherapy alone ⫽ 13.8 months vs 6.3 months,
modality of chemo and radiation therapies improved median OS in
P ⫽ .037). According to treatment modality, the presence of LTI
comparison with chemotherapy alone, problems of early relapse
unchangeably reduced 2-year OS (combined modality 22% vs
and mortality remained unresolved. In this study, LTI retained
82%, P ⬍ .001; and chemotherapy alone 7% vs 74%, P ⬍ .001;
predictive capacity of OS and DFS in treatment modality–adjusted
multivariate analyses. Nevertheless, the heterogeneity of treatmentmight weaken the prognostic significance of LTI.
Our study showed the adverse survival outcome of high IPI
Table 2. Clinical factors influencing overall survival
score, consistent with other previous reports.13,19 However, IPI lost
in univariate analysis
the predictive capacity of DFS in multivariate analysis because
Table 3. Clinical factors influencing overall survival
IPI score of 2 or higher
in multivariate analysis
No. of extranodal sites of 2 or more
Age older than 60 years
ECOG PS of 2 or higher
Presence of B symptoms
IPI score of 2 or higher
BLOOD, 1 DECEMBER 2005
LOCAL TUMOR INVASIVENESS IN NK/T-CELL LYMPHOMA
䡠 VOLUME 106, NUMBER 12
Table 4. Characteristics of 23 patients with local tumor invasiveness
Response to
OS (DFS),
Age, y/sex
Sites of LTI
Tx indicates treatment modality; M, male; CTX, chemotherapy alone; L, local failure; DOD, died of disease; F, female; PD, progressive disease; S, systemic failure; NE, not
evaluable; TRM, treatment-related mortality; PR, partial remission; CM, combined modality; and R, regional failure.
only 2 IPI factors had univariate association with DFS. Nonethe-
In this study, chemotherapy alone deteriorated OS, DFS, and the
less, in a nationwide survey of 326 Korean patients, IPI was a
probability of achieving CR in patients with nasal stage IE/IIE NTCL and
significant prognostic factor when patients with stage IIIE/IVE were
decreased median OS in patients with LTI. Since no patients with LTI
included.13 Although most studies to date have found the Ann
were treated with radiation therapy alone, we could cautiously conclude
Arbor stage to be an independently significant prognostic factor
that combined modality is superior to chemotherapy alone for improv-
predictive of survival,14,16,18,23,26,28,30 the staging system failed to
ing OS. However, the intrinsic problems of analysis that included
predict OS, DFS, and probability of achieving CR in this study as
heterogeneous chemotherapy regimens and treatment modalities re-
well as in the previously reported multicenter collaborative study
mained unresolved. Therefore, it is not possible to draw meaningful
of 326 Korean patients.13 Such discrepancies may be a result of
conclusions on the optimal treatment modality and the role of radiation
false-positive benign lymphoproliferative nodes associated with
therapy in patients with LTI.
EBV in patients with Ann Arbor stage IIE.
The presence of B symptoms was an independently significant
In terms of treatment modality, it has been demonstrated that
factor for the low probability of achieving CR in our study, which
treatment with radiotherapy improved survival28 but addition of
was explored as a prognostic factor in previous studies.18,28,31
anthracycline-based regimens had no proven role.28,31 Early radio-
Rather, advanced age predicted reduced OS and DFS in univariate
therapy32 and additional booster radiotherapy16 were emphasized
and treatment modality–adjusted multivariate analyses, respec-
by a few investigators to reduce local failure. Two studies
tively. However, the presence of B symptoms and advanced age
suggested the need for systemic chemotherapy in addition to
should be further investigated as prognostic factors.
radiation therapy to resolve the problem of frequent systemic
The status of EBV RNA failed to predict response and survival,
failures in patients receiving radiation therapy alone.30,32 However,
but EBV RNA positivity had a tendency to reduce OS and DFS in
high expression of multidrug resistance protein 1 mRNA or its
our study; however, due to the limited number of EBV RNA tests,
product, P glycoprotein, has led to resistance to chemotherapy and
its significance is inconclusive on survival. Recently, Au et al35
aggressive tumor behavior.33 In trying to tackle chemo-resistance,
showed that plasma EBV DNA at presentation correlated with
autologous stem cell transplantation was attempted, which if
stage and LDH level but did not correlate with IPI in 23 patients
performed in the first CR showed a trend toward better OS
with NTCL. High-presentation EBV DNA was the most significant
compared with historic controls.34
prognostic factor for reduced DFS and showed a trend of nega-tively affecting OS. Furthermore, there was evidence that cytotoxic
Table 5. Comparison of overall survival according to local
molecules, such as perforin, granzyme B, and Fas ligand, produced
tissue damage that was also induced by angiocentricity.36 Therefore,
2-year OS, %
we should observe the correlation of LTI with plasma EBV DNA
and also find cytotoxic molecules associated with LTI in the future.
Chemotherapy alone
In conclusion, this study demonstrated the importance of LTI as
Combined modality
a prognostic factor in nasal stage IE/IIE NTCL. Ann Arbor stage
LTI⫺ indicates absence of LTI; LTI⫹, presence of LTI.
dose not seem to predict survival and IPI lost predictive capacity of
BLOOD, 1 DECEMBER 2005 䡠 VOLUME 106, NUMBER 12
DFS in multivariate analysis. Consequently, LTI is the mostimportant prognostic factor in nasal stage IE/IIE NTCL. Future
efforts should be directed toward finding optimal treatment modali-ties including combined modality in managing patients with local
We acknowledge the assistance of Sun Young Yum, MD, for
tumor invasiveness.
revising the manuscript.
1. Carbone PP, Kaplan HS, Musshoff K, et al. Re-
13. Lee SY, Park K, Ryoo BR, et al. Korean multi-
26. Li YX, Coucke PA, Li JY, et al. Primary non-
port of the committee on Hodgkin's disease stag-
center study of extranodal NK/T-cell lymphoma:
Hodgkin's lymphoma of the nasal cavity: prog-
ing classification. Cancer Res. 1971;31:1860-
failure of Ann Arbor staging in predicting progno-
nostic significance of paranasal extension and
sis [abstract]. Int J Hematol. 2002;76(suppl 1):27.
the role of radiotherapy and chemotherapy. Can-
2. Rosenberg SA. Validity of the Ann Arbor staging
14. Cheung MM, Chan JK, Lau WH, et al. Primary
classification for the non-Hodgkin's lymphomas.
non-Hodgkin's lymphoma of the nose and naso-
27. You JY, Chi KH, Yang MH, et al. Radiation
Cancer Treat Rep. 1977;61:1023-1027.
pharynx: clinical features, tumor immunopheno-
therapy versus chemotherapy as initial treatment
3. Danieu L, Wong G, Koziner B, et al. Predictive
type, and treatment outcome in 113 patients.
for localized nasal natural killer (NK)/T-cell lym-
model for prognosis in advanced diffuse histio-
J Clin Oncol. 1998;16:70-77.
phoma: a single institute survey in Taiwan. Ann
cytic lymphoma. Cancer Res. 1986;46:5372-
15. King AD, Lei KI, Ahuja AT, et al. MR imaging of
nasal T-cell/natural killer cell lymphoma. AJR
28. Cheung MM, Chan JK, Lau WH, et al. Early stage
4. Shipp MA, Harrington DP, Anderson JR, et al. A
Am J Roentgenol. 2000;174:209-211.
nasal NK/T-cell lymphoma: clinical outcome,
predictive model for aggressive non-Hodgkin's
16. Koom WS, Chung EJ, Yang WI, et al. Angiocen-
prognostic factors, and the effect of treatment
lymphoma: The International Non-Hodgkin's Lym-
tric T-cell and NK/T-cell lymphomas: radiothera-
modality. Int J Radiat Oncol Biol Phys. 2002;54:
phoma Prognostic Factors Project. N Engl J Med.
peutic viewpoints. Int J Radiat Oncol Biol Phys.
29. Kern WF, Spier CM, Hanneman EH, et al. Neural
5. Ansell SM, Habermann TM, Kurtin PJ, et al. Pre-
cell adhesion molecule-positive peripheral T-cell
17. Robbins KT, Fuller LM, Vlasak M, et al. Primary
dictive capacity of the International Prognostic
lymphoma: a rare variant with a propensity for
lymphomas of the nasal cavity and paranasal si-
Factor Index in patients with peripheral T-cell lym-
unusual sites of involvement. Blood. 1992;79:
nuses. Cancer. 1985;56:814-819.
phoma. J Clin Oncol. 1997;15:2296-2301.
18. Logsdon MD, Ha CS, Kavadi VS, et al. Lym-
6. Jaffe ES, Chan JK, Su IJ, et al. Report of the
30. Kim GE, Cho JH, Yang WI, et al. Angiocentric
phoma of the nasal cavity and paranasal sinuses:
Workshop on Nasal and Related Extranodal An-
lymphoma of the head and neck: patterns of sys-
improved outcome and altered prognostic factors
giocentric T/Natural Killer Cell Lymphomas: efini-
temic failure after radiation treatment. J Clin On-
with combined modality therapy. Cancer. 1997;
tions, differential diagnosis, and epidemiology.
col. 2000;18:54-63.
Am J Surg Pathol. 1996;20:103-111.
31. Kim WS, Song SY, Ahn YC, et al. CHOP followed
19. Chim CS, Ma SY, Au WY, et al. Primary nasal
7. Quintanilla-Martinez L, Franklin JL, Guerrero I, et
by involved field radiation: is it optimal for local-
natural killer cell lymphoma: long-term treatment
al. Histological and immunophenotypic profile of
ized nasal natural killer/T-cell lymphoma? Ann
outcome and relationship with the International
nasal NK/T cell lymphomas from Peru: high
Prognostic Index. Blood. 2004;103:216-221.
prevalence of p53 overexpression. Hum Pathol.
32. Ribrag V, Ell Hajj M, Janot F, et al. Early locore-
20. Cheson BD, Horning SJ, Coiffier B, et al. Report
gional high-dose radiotherapy is associated with
of an international workshop to standardize re-
8. Gaal K, Sun NC, Hernandez AM, et al. Sinonasal
long-term disease control in localized primary an-
sponse criteria for non-Hodgkin's lymphomas:
NK/T-cell lymphomas in the United States. Am J
giocentric lymphoma of the nose and nasophar-
NCI Sponsored International Working Group.
Surg Pathol. 2000;24:1511-1517.
ynx. Leukemia. 2001;15:1123-1126.
J Clin Oncol. 1999;17:1244-1253.
9. Kang YK, Kim BS, Kim TW, et al. Clinicopatho-
33. Drenou B, Lamy T, Amiot L, et al. CD3- CD56⫹
21. Kaplan EL, Meier P. Nonparametric estimation
logic characteristics of Korean Non-Hodgkin's
non-Hodgkin's lymphomas with an aggressive
from incomplete observation. J Am Stat Assoc.
lymphomas based on REAL classification. J Ko-
behavior related to multidrug resistance. Blood.
rean Cancer Assoc. 1999;31:641-652.
22. Cox DR. Regression models and life-tables. J R
10. Ko YH, Ree HJ, Kim WS, et al. Clinicopathologic
34. Au WY, Lie AK, Liang R, et al. Autologous stem
Stat Soc [B]. 1972;34:187-220.
and genotypic study of extranodal nasal-type
cell transplantation for nasal NK/T-cell lymphoma:
natural killer/T-cell lymphoma and natural killer
23. Liang R, Todd D, Chan TK, et al. Treatment out-
a progress report on its value. Ann Oncol. 2003;
precursor lymphoma among Koreans. Cancer.
come and prognostic factors for primary nasal
lymphoma. J Clin Oncol. 1995;13:666-670.
35. Au WY, Pang A, Choy C, et al. Quantification of
11. Harabuchi Y, Yamanaka N, Kataura A, et al. Ep-
24. Cuadra-Garcia I, Proulx GM, Wu CL, et al. Si-
circulating Epstein-Barr virus (EBV) DNA in the
stein-Barr virus in nasal T-cell lymphomas in pa-
nonasal lymphoma: a clinicopathologic analysis
diagnosis and monitoring of natural killer cell and
tients with lethal midline granuloma. Lancet.
of 58 cases from the Massachusetts General
EBV-positive lymphomas in immunocompetent
Hospital. Am J Surg Pathol. 1999;23:1356-1369.
patients. Blood. 2004;104:243-249.
12. Kanavaros P, Lescs MC, Briere J, et al. Nasal T-
25. Abbondanzo SL, Wenig BM. Non-Hodgkin's lym-
36. Ohshima K, Suzumiya J, Shimazaki K, et al. Na-
cell lymphoma: a clinicopathologic entity associ-
phoma of the sinonasal tract: a clinicopathologic
sal T/NK cell lymphomas commonly express per-
ated with peculiar phenotype and with Epstein-
and immunophenotypic study of 120 cases. Can-
forin and Fas ligand: important mediators of tis-
Barr virus. Blood. 1993;81:2688-2695.
sue damage. Histopathology. 1997;31:444-450.
2005 106: 3785-3790
originally published online
doi:10.1182/blood-2005-05-2056August 18, 2005
Local tumor invasiveness is more predictive of survival than
International Prognostic Index in stage I E E
/II extranodal NK/T-cell
lymphoma, nasal type
Tae Min Kim, Yeon Hee Park, Sang-Yoon Lee, Ji-Hoon Kim, Dong-Wan Kim, Seock-Ah Im, Tae-You
Kim, Chul Woo Kim, Dae Seog Heo, Yung-Jue Bang, Kee-Hyun Chang and Noe Kyeong Kim
Updated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
Information about reproducing this article in parts or in its entirety may be found online at:
Information about ordering reprints may be found online at:
Information about subscriptions and ASH membership may be found online at:
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Societyof Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Source: http://www.scure.co.kr/upload_file/pds/1458786917-TJMTL.pdf
Guido Clemente Solari Montenegro FACTORES DE RIESGO FÍSICO RELACIONADOS CON EL DOLOR LUMBAR: ANALISIS BIBLIOGRÁFICO DE LA SITUACION. PROF. DR. GUIDO C. SOLARI M. ACADEMICO, PROF. ASOCIADO DEPARTAMENTO DE KINESIOLOGIA UNIVERSIDAD DE ANTOFAGASTA 1.- Definición y Clasificación del SDL El lumbago o lumbalgia son términos que permiten hacer referencia al
Women's Health West Policy and Law Reform Scan This scan is provided to inform the WHW strategic planning process. It outlines key policy documents, legislative reforms and the external policy environment that relate to women's health, safety and wellbeing. © Women's Health West International Context International Gender Equality In November 2015, the United Nations Entity for Gender Equality and the Empowerment of Women (UN Women) held a 16-day international conference in Istanbul to end men's violence against women. Official representatives from more than 40 countries vowed to take a zero tolerance approach and immediate action to end the global epidemic of violence against women. They agreed to greater investment in gender equality, to share data on violence against women and to strengthen existing laws to protect women. The conference was held 20 years after the landmark Beijing Declaration and Platform for Action, which was adopted by 189 countries in 1995 and set the most progressive agenda for advancing women's rights. Since the conference, the Executive Directors of UN Women and UNFPA launched the Essential Services Package, a toolkit of guidelines, services and best practice to support women and girls subjected to violence. This resource can be found here: Canadian Prime Minister Justin Trudeau selects a 50-50 cabinet (2015) In November newly elected Canadian Prime Minister Justin Trudeau announced his cabinet which for the first time in Canadian history is made up of 15 men and 15 women. When asked at a press conference why he chose a gender balanced cabinet, the self-declared feminist's answer was brief: "Because it's 2015". The new gender division comes on top of existing cabinet-making criteria for regional, linguistic and ethnic representation, including the practice of selecting at least one minister from each of the country's 10 provinces. Trudeau's cabinet also includes a former Afghanistan refugee as the minister of democratic institutions, a para-Olympic swimmer from Vancouver in the sports ministry and an Aboriginal lawyer as minister of justice and attorney general. More details about Trudeau's cabinet can be found her Nepal's first female Prime Minister (2015) Nepal has elected a long-time women's rights campaigner as the country's first female president, as the Himalayan nation pushes for more gender equity in politics and civic life. Bidhya Devi Bhandari, the 54-year-old deputy leader of Nepal's Communist Party of Nepal Unified Marxist-Leninist, had lobbied actively for the new constitution to require that either the president or vice-president be a woman. Bidhya Devi Bhandari said her election by the Parliament marked a first step towards assuring these constitutional guarantees of equality are fulfilled. The constitution now requires that one-third of the country's legislators be women, and that women be included in all government committees. Bidhya Devi Bhandari has also promised to actively champion the rights of minority groups and women in Nepal. Global Ambassador for Women and Girls Former Democrats leader Natasha Stott Despoja has been appointed to this position by Foreign Minister, Julie Bishop. This follows her appointment as founding chair of the Foundation to prevent Violence against Women and their Children. The minister sees ‘one of the best ways to achieve peace and security and…achieve stronger communities and societies is to empower the women and the girls in your populations'. Further information can be found at: Trans Pacific Partnership negotiations (2013) Australia is currently participating in the final stages of negotiations for the Trans Pacific Partnership; an agreement to regulate free trade in the Asia-Pacific region. While the details of the agreement are yet to be released, a draft of the intellectual property chapter was leaked in November 2013. United States draft proposals for expanded patent protection have led many academics and public health professions to question what the agreement might mean for timely access to affordable medicines. In response, a motion was passed in the senate calling for early release of the draft text and greater public scrutiny of the agreement. The following areas of concern were raised in the letter presented to the federal Minister for Health by 44 prominent academics in public health and health sciences: