Kamagra gibt es auch als Kautabletten, die sich schneller auflösen als normale Pillen. Manche Patienten empfinden das als angenehmer. Wer sich informieren will, findet Hinweise unter kamagra kautabletten.
030515 identification of a novel coronavirus in patients with severe acute respiratory syndrome
The new england journal
of medicine
Identification of a Novel Coronavirus in Patients
with Severe Acute Respiratory Syndrome
Christian Drosten, M.D., Stephan Günther, M.D., Wolfgang Preiser, M.D.,
Sylvie van der Werf, Ph.D., Hans-Reinhard Brodt, M.D., Stephan Becker, Ph.D.,
Holger Rabenau, Ph.D., Marcus Panning, M.D., Larissa Kolesnikova, Ph.D.,
Ron A.M. Fouchier, Ph.D., Annemarie Berger, Ph.D., Ana-Maria Burguière, Ph.D.,
Jindrich Cinatl, Ph.D., Markus Eickmann, Ph.D., Nicolas Escriou, Ph.D.,
Klaus Grywna, M.Sc., Stefanie Kramme, M.D., Jean-Claude Manuguerra, Ph.D.,
Stefanie Müller, M.Sc., Volker Rickerts, M.D., Martin Stürmer, Ph.D., Simon Vieth,
Hans-Dieter Klenk, M.D., Albert D.M.E. Osterhaus, Ph.D.,
Herbert Schmitz, M.D., and Hans Wilhelm Doerr, M.D.
b a c k g r o u n d
The severe acute respiratory syndrome (SARS) has recently been identified as a new From the Bernhard Nocht Institute for Trop-
ical Medicine, National Reference Center
clinical entity. SARS is thought to be caused by an unknown infectious agent.
for Tropical Infectious Diseases, Hamburg(C.D., S.G., M.P., K.G., S.K., S.M., S.V.,
H.S.); the Institute of Medical Virology(W.P., H.R., A.B., J.C., M.S., H.W.D.) and the
Clinical specimens from patients with SARS were searched for unknown viruses with Medical Clinic III (H.-R.B., V.R.), Johann
the use of cell cultures and molecular techniques.
Wolfgang Goethe University, Frankfurt amMain; and the Institute of Virology, Phil-ipps University, Marburg (S.B., L.K., M.E.,
H.-D.K.) — all in Germany; the Pasteur In-
A novel coronavirus was identified in patients with SARS. The virus was isolated in cell stitute, Molecular Genetics of Respiratoryculture, and a sequence 300 nucleotides in length was obtained by a polymerase-chain- Tract Viruses, National Influenza Center
(Northern France), Paris (S.W., A.-M.B.,
reaction (PCR)–based random-amplification procedure. Genetic characterization in- N.E., J.-C.M.); and the Institute of Virology,
dicated that the virus is only distantly related to known coronaviruses (identical in 50 to Erasmus University, Rotterdam, the Neth-60 percent of the nucleotide sequence). On the basis of the obtained sequence, conven- erlands (R.A.M.F., A.D.M.E.O.). Address
reprint requests to Dr. Drosten at the De-
tional and real-time PCR assays for specific and sensitive detection of the novel virus partment of Virology, Bernhard Nocht
were established. Virus was detected in a variety of clinical specimens from patients Institute for Tropical Medicine, Bernhard-with SARS but not in controls. High concentrations of viral RNA of up to 100 million Nocht Str. 74, 20359 Hamburg, Germany,
or at
[email protected].
molecules per milliliter were found in sputum. Viral RNA was also detected at extremelylow concentrations in plasma during the acute phase and in feces during the late con- Drs. Drosten and Günther contributedvalescent phase. Infected patients showed seroconversion on the Vero cells in which equally to this article.
the virus was isolated.
This article was published at www.nejm.orgon April 10, 2003.
N Engl J Med 2003;348:1967-76.
The novel coronavirus might have a role in causing SARS.
Copyright 2003 Massachusetts Medical Society.
n engl j med 348;20
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
The new england journal
of medicine
he severe acute respiratory syn-
developed on day 2. The temperature decreased dur-
drome (SARS) was recently identified as a ing days 5 and 6, but on day 7 fever developed again
tnew clinical entity.1,2 Patients present with and there were crackles over her lungs, accompa-
fever, dry cough, dyspnea, headache, and hypox- nied by dry cough and hypoxemia (partial pressureemia. Typical laboratory findings are lymphopenia of oxygen in arterial blood, 65 mm Hg). Convales-and mildly elevated aminotransferase levels. Death cence began on day 9. Laboratory abnormalities in-may result from progressive respiratory failure due cluded a maximal C-reactive protein level of 1.5 mgto alveolar damage.3 SARS appears to be caused by per deciliter, leukopenia, and lymphopenia. Ther-an unknown infectious agent that is transmitted apy comprised erythromycin and ceftriaxone.
from human to human. The World Health Organi-
Contact 2, the mother of Contact 1, had head-
zation (WHO) had recorded 2353 cases by April 4, ache and myalgia on March 13 (day 1) and sore2003. About 4 percent of patients with SARS have throat and fever (temperature, 38.2°C) on day 2. Fe-died.4 The SARS epidemic started in Asia, with the ver disappeared on day 3. She reported burning painmajority of cases occurring in China and the Asia– in the eyes on days 4 and 5. There were no patholog-Pacific region. The epidemic has spread from Asia to ic findings on chest radiography. Pathologic labo-other continents through international travel. The ratory findings included a maximal C-reactive pro-WHO has established a network of international tein level of 9.9 mg per deciliter, an increase in thelaboratories to facilitate the identification of the aspartate aminotransferase level to 154 U per liter,causative agent of SARS. As part of this network, and an increase in the lactate dehydrogenase levelwe have identified and characterized a novel coro- to 319 U per liter between days 9 and 16. Therapynavirus in patients with SARS.
involved imipenem, levofloxacin, doxycycline, andoseltamivir.
A total of 49 specimens from 18 patients with
suspected or probable SARS, according to the WHO
case definition, and from 21 healthy contact per-
The index patient was a 32-year-old male physician. sons were sampled between March 5 and March 27,
From March 3 to 9, 2003, he treated a patient with 2003, during the SARS epidemic in Hanoi, Viet-
atypical pneumonia in Singapore who had arrived nam.2 A total of 54 stool samples from patients in
from Hong Kong. On March 9 (day 1) his illness Germany were available as controls.
started with abrupt onset of fever (temperature,
39.4°C), when he was in New York. On day 4, a dry
microbiologic and virologic testing for
cough and a sore throat developed, along with
typical and atypical respiratory pathogens
erythema on the trunk. During a stopover in Frank- Respiratory and blood specimens from the patients
furt, Germany, on his flight to Singapore, he was in Frankfurt were tested by polymerase chain reac-
transferred to an isolation unit at the Frankfurt Uni- tion (PCR) with specific primers for
Mycoplasma
versity Hospital with suspected SARS (day 7). He had
pneumoniae, Chlamydia pneumoniae, human cytomeg-
hypoxemia (partial pressure of oxygen in arterial alovirus, adenoviruses, respiratory syncytial virus,
blood, 59 mm Hg) and required oxygen supple- parainfluenzavirus types 1, 2, 3, and 4, Hendra vi-
mentation. Chest radiography showed worsening rus, Nipah virus, human metapneumovirus, influ-
bilateral opacifications. Laboratory abnormalities enzaviruses A and B, rhinovirus, and human coro-
included elevated levels of aspartate aminotrans- navirus strains OC43 and 229E, as well as with
ferase (46 U per liter) and lactate deydrogenase universal primers for herpesviruses, arenaviruses,
(478 U per liter) and an elevated maximal C-reac- bunyaviruses, enteroviruses, alphaviruses, flavivi-
tive protein level (30.7 mg per deciliter), as well as ruses, filoviruses, and paramyxoviruses. Respiratory
leukopenia and lymphopenia. Convalescence began specimens were also tested by antigen enzyme-
on day 10. Treatment involved levofloxacin, vanco- linked immunosorbent assay (ELISA) for
M. pneu-
mycin, imipenem, doxycycline, and oseltamivir.
moniae, influenzaviruses A and B, and respiratory
Two contacts of the index patient (Contacts 1 and syncytial virus. Antigen ELISA for legionella species
2) were isolated as well. Contact 1, the patient's was performed with urine. Paired serum sampleswife, reported a headache after admission (March were tested serologically for
C. pneumoniae (IgA and15, day 1). Fever (temperature, 38.2°C) and myalgia IgG),
C. trachomatis (IgA and IgG),
C. psittaci (IgG),
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
M. pneumoniae, Coxiella burnetii, influenzaviruses A Products were sequenced with the use of a didesoxyand B (IgG and IgA), dengue virus (IgG and IgM), terminator sequencing reaction (BigDye termina-measles virus (IgG and IgM), hantaviruses, adeno- tor reaction mix, Applied Biosystems) and an auto-viruses, parainfluenzavirus types 1, 2, and 3, and mated DNA sequencer (model 3100, Applied Bio-respiratory syncytial virus.
Electron microscopy was performed with nega-
tive staining of respiratory and blood samples. In
rt-pcr specific for the novel coronavirus
addition, cells in bronchoalveolar-lavage fluid were For diagnostic RT-PCRs, the Superscript II platinum
analyzed with the use of ultrathin sections embed-
Taq polymerase one-step RT-PCR kit was used. De-
ded in Epon and LR Gold resins. Vero, Madin–Derby tails of the procedures are summarized in Table 1.
canine-kidney, and A549 cells were inoculated with An RNA standard transcribed in vitro was generat-
respiratory and blood specimens from all three pa- ed by amplification of the target region with primers
tients and grown under biosafety level 3 or 4 condi- BNIoutS2 and BNIoutAs. The fragment was cloned
tions.
and transcribed into RNA in vitro, essentially as de-scribed elsewhere.5
Sputum samples were shaken for 30 minutes with
sequence and phylogenetic analysis
an equal volume of acetylcysteine (10 g per liter) We searched for homologies to known sequences
and 0.9 percent sodium chloride. The resulting ho- using the nucleotide or translated data base of the
mogenate, native body fluids, resuspended swab Basic Local Alignment Search Tool (BLAST) at http:
samples (in 1 ml of phosphate-buffered saline), or //www.ncbi.nlm.nih.gov:80/BLAST/. Phylogenetic
tissue-culture supernatant was extracted with a viral analysis was performed with the use of the Phyloge-
RNA kit (QIAamp, Qiagen; elution volume, 60 µl). ny Inference Package (PHYLIP), version 3.57c.6
Stool specimens were extracted with the QIAamp
stool kit (Qiagen).
p r o c e d u r e
p a t h o g e n s
A volume of 2 µl of RNA solution was analyzed with A large number of tests for known respiratorya random reverse-transcriptase (RT)–PCR assay. The pathogens were performed with specimens from allSuperscript II platinum
Taq polymerase one-step three patients in Frankfurt. The test results wereRT-PCR kit (Invitrogen) was used for the reaction negative, except as follows.
(20 µl total volume). Reactions contained 10 µl of
Paramyxovirus-like particles were seen in throat
buffer concentrate, 2 mM of magnesium sulphate, swabs and sputum samples from the index patient0.8 µl of enzyme mixture, and 1.9 µM of each of two by electron microscopy. The particles were scarce.
primers. Fifteen primer pairs were used. Some of the However, several PCR tests specific for virus speciesprimers contained degenerate positions, and most of the family Paramyxoviridae were negative (includ-had a thymidine residue at their 3' ends to allow ing tests for human metapneumovirus), as wereDNA polymerase to work in spite of incomplete PCR assays based on primers designed to reactnucleotide matches at the ends of the primers.4 broadly with all members of that family. The primers were originally designed to target the
C. pneumoniae was not detected by PCR or antigen
genome of yellow fever virus strain 17D and the ELISA in sputum of the index patient from day 9.
polymerase gene of Paramyxoviridae. Thermal cy- However, on day 11, electron microscopy of cells incling comprised 42°C for 30 minutes; 95°C for a bronchoalveolar-lavage specimen from the index3 minutes; 10 cycles of 95°C for 10 seconds, 55°C patient showed a severe intracellular bacterial infec-for 15 seconds (decreasing by 1°C per cycle), 72°C tion, and the bronchoalveolar-lavage cells reacted infor 40 seconds; 40 cycles of 95°C for 10 seconds, immunofluorescence analyses with a monoclonal56°C for 10 seconds, and 72°C for 40 seconds. Prod- antibody directed against
C. pneumoniae. Consistentucts were analyzed on a 1 percent agarose gel, gel- with this finding, there was an increase by a factorpurified, and reamplified with the use of the corre- of four in the
C. pneumoniae IgA titer in the index pa-sponding primers but without degenerate positions. tient between day 10 and day 13.
n engl j med 348;20
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
The new england journal
of medicine
Table 1. Primers and Protocols for Diagnostic Polymerase-Chain-Reaction Assays.
Target and Fragment Length
Thermal Cycling Profile
ggg TTg ggA CTA TCC
10 µl 2¬ reaction buffer†
2.45 mM magnesium sulfate†
500 nM each primer
0.4 µl reverse-transcriptase/
60°C, 10 sec (decrease
Taq DNA polymerase
by 1°C per cycle)
CCA TCA TCA gAT AgA
20 µl total volume
for protocols 1 and 2
5 µl 10¬ reaction buffer‡
2.5 mM magnesium chloride‡
200 nM each primer
60°C, 10 sec (decrease
1.25 units platinum
Taq
by 1°C per cycle)
nested PCR for protocol 3
1 µl PCR product from previ-
50 µl total volume
12.5 µl 2¬ reaction buffer†
3.6 mM magnesium sulfate†
1 µg bovine serum albumin§
200 nM each primer
0.6 µl reverse-transcriptase/
Taq DNA polymerase
Fluorescence measured
TCg TgC gTg gAT Tgg
25 µl total volume
* Sequence was communicated through the World Health Organization's SARS etiology network by colleagues from the Centers for Disease Control
and Prevention (CDC).
† Formulation was included in the Superscript II reverse transcriptase (RT)/platinum
Taq polymerase one-step RT-PCR kit (Invitrogen).
‡ Formulation was supplied with platinum
Taq DNA polymerase (Invitrogen).
§ Formulation was supplied by Sigma.
¶ Fluorescence was measured with the Roche LightCycler, F1 detection channel, and the Applied Biosystems 7000 SDS machine, FAM detection
channel without passive reference dye.
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
The novel coronavirus isolate was termed FFM-ic
(for Frankfurt am Main index case).
After six days of incubation (on March 21), a cyto-
To compare our isolate with that obtained by the
pathic effect was seen on Vero-cell cultures inocu- CDC, a fragment corresponding to the CDC frag-lated with sputum obtained from the index patient ment was amplified from the cell-culture superna-on day 7. Twenty-four hours after a single passage, tant and sequenced. Both sequences were 100 per-nucleic acids were purified from the supernatant. cent identical. Next, primers specifically targetingRandom amplification was performed with 15 dif- the BNI-1 fragment and the CDC fragment wereferent PCRs under low-stringency conditions. We synthesized. With the use of a long-range PCR pro-had previously shown that this method is able to tocol,8 a region extending from the CDC fragmentdetect unknown pathogens growing in cell culture to the BNI-1 fragment was amplified. The obtained(unpublished data). To detect RNA viruses, an ini- fragment had the expected length of 3 kb. It was se-tial reverse-transcription step was included.
quenced from both ends, and the sequences were
About 20 distinct DNA fragments were obtained found to be identical to the CDC and BNI-1 se-
and sequenced. The resulting sequences were sub- quences, respectively, demonstrating that the two
jected to BLAST data-base searches. Most of the sequences were derived from a contiguous RNA
fragments matched human chromosome sequenc- molecule and, thus, from the same virus. Since the
es, indicating that genetic material of the cultured same virus was isolated from two independent cas-
cells had been amplified (Vero cells are derived from es of SARS, and since there was serologic evidence
monkeys). Three of the fragments did not match of an acute infection with this virus in our index pa-
any nucleotide sequence in the data base. However, tient and also in Contact 1 (as described below), it
when a translated BLAST search was performed was considered that the coronavirus might have a
(comparison of the amino acid translation in all six role in causing SARS. Specific diagnostic assays
possible reading frames with the data base), these were therefore established for the detection of the
fragments showed homology to coronavirus amino pathogen.
acid sequences, indicating that a coronavirus had
been isolated. Two of the fragments were 300 nucle-
establishment of diagnostic pcr assays
otides in length and identical in sequence, and the
targeting the bni-1 fragment
third fragment was 90 nucleotides in length (se- A nested set of primers was designed within the
quences BNI-1 and BNI-2, respectively, as reported BNI-1 fragment (Fig. 1B). The outer set of primers
on the Web site of the WHO network on March 25) (protocol 3) (Table 1) detected the virus in clinical
(Fig. 1A). Detailed sequence analysis revealed that specimens from the index patient and Contact 1,
both fragments were located in the open reading who also had clinical signs of SARS (Table 2). Ad-
frame 1b of coronaviruses and did not overlap with ditional specimens were positive on nested RT-PCR
a 400-nucleotide coronavirus fragment identified (protocols 3 plus 5) (Tables 1 and 2). (The avail-
by colleagues at the Centers for Disease Control ability of PCR protocols at http://www.bni.
and Prevention (CDC) (sequence CDC, reported on uni-hamburg.de/ was reported to the WHO network
the Web site of the WHO network on March 24) on March 27 and to ProMed mail [an international
(Fig. 1A).
e-mail notification service for infectious-disease
There were sequences of six coronaviruses of all outbreaks] on March 30.) To have a practical and
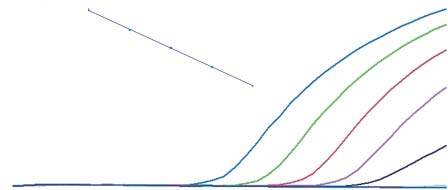
phylogenetic lineages (groups 1, 2, and 3) in the se- quantitative test, a real-time RT-PCR with a 5'-quence data base that overlapped with sequences nuclease probe was established (protocol 6) (Ta-BNI-1 and BNI-2. All known sequences were only ble 1 and Fig. 1B). After optimization with the usedistantly related to the new sequences (Fig. 1B). of quantified RNA transcribed in vitro, the assay re-The BNI-1 nucleotide sequence diverged from the liably detected 10 copies of RNA per reaction, cor-known sequences by between 39 percent (bovine responding to 830 RNA molecules per milliliter ofcoronavirus) and 46 percent (porcine epidemic di- specimen (Fig. 2). The sensitivities of nested andarrhea virus). Such distances are typically found be- real-time PCR were equivalent (Table 2). The spec-tween different genetic lineages of coronaviruses.7 ificity of the PCR with outer primers, of the nestedA stable phylogeny was obtained with the BNI-1 PCR, and of the real-time PCR (protocols 3, 3 plus 5,fragment, indicating that the isolated coronavirus and 6, respectively) (Table 1) was tested with the usesegregates between genetic groups 2 and 3 (Fig. 1C). of RNA purified from cultures of bovine coronavi-
n engl j med 348;20
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
The new england journal
of medicine
rus, avian infectious coronavirus, porcine transmis-sible gastroenteritis coronavirus, and human coro-
Figure 1 (facing page). Genetic Characterization of the
Novel Coronavirus.
naviruses 229E and OC43. None of the PCR assays
Panel A shows a schematic representation of coronavi-
cross-reacted with these viruses — a finding that is
rus genome organization (with bovine coronavirus, ac-
consistent with their considerable genetic differenc-
cession number NC_003045, as an example). Genes are
es from the novel coronavirus.
depicted by brown arrows pointing in the direction of
Quantification of the viral RNA concentration in
translation. Vertical arrows indicate the genomic location
clinical specimens from the index patient and Con-
of the sequence fragments of the novel coronavirus found by the CDC and in our study (BNI-1 and BNI-2).
tact 1 by real-time PCR revealed that the highest con-
UTR denotes untranslated region, orf open reading
centration — as high as 100 million copies per mil-
frame, NS nonstructural protein, HE hemagglutinin-
liliter — was present in sputum (Table 2). After
esterase glycoprotein, S spike glycoprotein, E small
enrichment of virus by ultracentrifugation, viral
membrane gene, M membrane glycoprotein, and
RNA was also detected in the serum of the index
N nucleoprotein.
patient, indicating the presence of low-level viremia
The top part of Panel B shows the nucleotide-sequence alignment of fragment BNI-1 with known coronaviruses.
during symptomatic disease. Both the index patient
The lower part of Panel B shows the amino acid–sequence
and Contact 1 had viral RNA in stool samples ob-
alignment of fragment BNI-1 with known coronaviruses.
tained during late convalescence, suggesting that
The nucleotide sequence was translated into single-letter
virus may be shed in feces for prolonged periods.
amino acid code. Bovine-CV denotes bovine coronavirus,
To investigate whether the novel coronavirus was
avian-IBV avian infectious bronchitis virus, murine-HV murine hepatitis virus, porcine-TGEV porcine transmis-
prevalent in patients in Germany who had gastro-
sible gastroenteritis coronavirus, porcine-EDV porcine
intestinal symptoms, a collection of 54 stored
epidemic diarrhea virus, and human CV-229E human
stool samples was tested with the use of the real-
coronavirus 229E. A dot indicates that the position is
time RT-PCR assay. None of the samples tested
identical to the reference sequence (BNI-1). The oligonu-
cleotides for the nested reverse-transcriptase polymer-ase chain reaction (RT-PCR, brown) and the real-time
The established PCR assays have also been used
RT-PCR (purple) are shown as arrows pointing in the
to test respiratory samples from German patients
direction of their elongation.
with symptoms and a travel history compatible with
In Panel C, a phylogenetic tree shows relations among
SARS. So far, 67 samples from 55 patients have been
coronavirus polymerase gene fragments (corresponding
tested. One patient fulfilling the WHO criteria for
to BNI-1) according to the neighbor-joining method. The
probable SARS was coronavirus-positive on PCR.
maximum likelihood method revealed the same rela-tions (data not shown). Genetic distances are indicated
PCR protocols, as well as positive control material,
by the lengths of the branches. Analyses were performed
have been made available to laboratories worldwide.
on a bootstrapped data set (100 replicates). In addition to the coronavirus isolate FFM-ic, avian infectious bron-
chitis virus (IBR31131), bovine coronavirus (AF220295), human coronavirus 229E (12175745), murine hepatitis
virus (9629812), porcine epidemic diarrhea virus
To provide evidence for the hypothesis that the nov-
(19387576), and porcine transmissible gastroenteritis
el coronavirus is associated with SARS, further spec-
coronavirus (13399293) were included in the analysis.
imens from patients with probable and suspected
SARS, as well as healthy contacts of patients affected
by the SARS epidemic in Hanoi, Vietnam, were test- evidence of an epidemiologic link among these pa-
ed by nested PCR assays targeting the CDC and tients. Furthermore, these findings suggest that the
BNI-1 fragments (protocols 2 plus 4 and 3 plus 5, virus is rather stable genetically.
respectively) (Table 1). The prevalence of the virus
was 100 percent among patients with probable cas-
serologic response
es of SARS and 23 percent among those with sus- The serologic response to the coronavirus was test-
pected cases of SARS, whereas virus was not detect- ed by a standard immunofluorescence technique
ed at all in the healthy contacts (Table 3). These with serial serum samples from all three patients
preliminary data may point to an association be- and coronavirus FFM-ic–infected Vero cells. Spe-
tween the novel coronavirus and SARS. A total of cific IgG was not detected in serum from the index
15 of the PCR products were sequenced — 7 from patient and Contact 1 until day 9 and day 10, re-
the CDC fragment and 8 from the BNI-1 fragment. spectively. Thereafter, the IgG titer increased to
All sequences were 100 percent identical to the cor- 1:1500 in the index patient and 1:250 in Contact 1.
responding CDC and BNI-1 sequences, providing No antibody response developed in Contact 2.
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
Human-CV-229E .TGAACATG .G.T.ATA T. GGT.TG.G TTAGCA.GCC .AGT.A. G.T.CT GT.TA.A. CTTT.C.G .T.CAPorcine-EDV
Human-CV-229E .A.GT.T. A.AA.G. G.A.TG CA.TC. AG.T.CAA. T.C. TG. A.AG.T.T .C.AT. G.T.
Porcine-EDV
Human-CV-229E T.CA. TGAA. G.CTA. AA.C.C.GG. GT.TTG.A. AACCT.CG .TCGTG.A .T.A. A.A.C.C T.CA.G.
Porcine-EDV
Amino acid sequences
Human-CV-229E .EHV.Y. RFDVSMP.SH SL.C.DF.M .G.L.M. A.V.G.N .V.V. N.DF.Q .E.C.L.NTG SVVKP.R.RA .E.T.IVPorcine-EDV
Murine hepatitis virus
Porcine transmissible
Bovine coronavirus
Human coronavirus 229E
Avian infectious bronchitis virus
n engl j med 348;20
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
The new england journal
of medicine
Table 2. Detection of the Novel Coronavirus in Various Clinical Specimens with the Use of Different PCR Assays.*
Result on PCR Assay
Throat swab, day 9
Nasal swab, day 9
Contact 1
Throat swab, day 3
Nasal swab, day 3
Contact 2
* PCR denotes polymerase chain reaction, BAL bronchoalveolar-lavage fluid, and ND not done. Plus signs indicate posi-
tive results, and minus signs negative results.
† Values are copies per milliliter. ‡ Sample was tested 24 hours after passage. § Test was positive but below the limit of reliable quantification (800 copies per milliliter).
¶ Test was performed after ultracentrifugation of 2 ml of plasma.
of this novel virus. The involvement of a coronavirus
in a respiratory disease would not be without prec-
The principal finding of the study is the identifica- edent: the two human coronaviruses are known totion of a novel coronavirus in patients with SARS. It cause mild respiratory illness.9 One should bear inappears that patients with SARS are acutely infected mind, however, that in the past, viruses have beenwith this virus, since they have virus-specific IgG initially isolated from patients with a specific dis-seroconversion. The high rate of positivity among ease but subsequent investigations revealed no actu-patients with probable cases during an outbreak of al association at all.10,11 Thus, larger studies withSARS in Hanoi, in conjunction with the complete appropriate control groups are needed to verify ornegativity among all healthy contacts of patients eliminate our hypothesis about the cause of SARS.
affected by the same outbreak, provides evidence of The assays that have been established provide anan association between the disease and the presence excellent tool for such studies. It should also be
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
taken into account that antigen that was present inprimary cultures was used to detect the antibody
response, and it remains to be firmly established
that this response is indeed directed against the
novel coronavirus rather than against an unknown
agent that might have been isolated simultaneous-
ly. This possibility could be tested with the use of
Log Copies of
plaque-purified virus or recombinant proteins as
RNA per Reaction
Fluorescence (arbitrary units)
By testing for a broad range of known pathogens,
we also obtained evidence for infection with para-
PCR Cycle
myxoviruses and C. pneumoniae. Paramyxoviruses —
Figure 2. Real-Time Polymerase Chain Reaction (PCR) Targeting the BNI-1
in particular, human metapneumovirus, which was
Fragment of the Novel Coronavirus.
previously implicated in SARS12 — could be largely
The plot shows an amplification of a limiting-dilution series of standard RNA
ruled out by further investigation. Infection with
transcribed in vitro. The y axis indicates the fluorescence signal recorded in
chlamydia was confirmed in several assays. Howev-
each amplification cycle, as plotted along the x axis. Numbers at the right
er, chlamydia was not found in other patients with
show the number of copies of RNA per reaction. The inset graph presents a standard curve showing the relation between the concentration in standard
SARS.3 Hence, it remains unclear whether these
samples (on the x axis) and the number of cycles it took to generate a fluores-
pathogens have a role as causative factors or cofac-
cence signal in the respective samples (on the y axis). The standard curve al-
lows quantification of coronavirus RNA in clinical samples.
The quantitative analysis of various clinical spec-
imens from the patients with SARS reveals interest-ing features of the viral infection. First, the viralRNA concentration in sputum was high in both pa-tients, suggesting that shedding of the virus from
Table 3. Proportion of Patients with a Positive RT-PCR Result for Coronavirus.*
the respiratory tract could be the primary route of
transmission. The extremely high RNA concentra-
of Samples
Fraction of Patients Testing
tions found in sputum from the index patient would
per Patient
be consistent with a high level of contagiousness ofthe SARS agent. The detection of low amounts of vi-
ral RNA in serum from the index patient on day 9
would be compatible with a long viremic phase,
suggesting that replication does not occur only in
Patients with probable SARS †
the respiratory tract. The elevated levels of aspartate
Patients with suspected SARS‡
aminotransferase and lactate dehydrogenase3 in-deed suggest that the agent causing SARS is also
replicating outside the respiratory tract. The pres-ence of viral RNA in stool of the patients late during * RT-PCR denotes reverse-transcriptase polymerase chain reaction.
† Samples were from the lower respiratory tract in five patients and nasopharyn-
convalescence is reminiscent of characteristics of
geal swabs in one patient (all positive); samples were obtained 3 to 13 days
other coronaviruses.13 Shedding of the virus in feces
after the onset of illness.
may be an additional source of spreading, provided ‡ Nasopharyngeal samples from 13 patients were used; they were obtained 3 to
12 days after the onset of illness.
that the virus is stable in this environment. From adiagnostic point of view, it is important to note thatnasal and throat swabs seem less suitable for diag- Vietnam, for providing specimens from and clinical data for their
nosis, since these materials contain considerably patients; to Britta Liedigk, Gaby Bauer, Marhild Kortenbusch, Valérieless viral RNA than sputum, and the virus may es- Lorin, Claudine Rousseaux, Maryse Tardy-Panit, Saliha Azebi, Chris-cape detection if only these materials are tested.
tophe Batejat, Gilberte Coralie, and Aurélien Brionne for excellenttechnical assistance; to Uli Lass, Christina Schiel, and Olfert Landt
Supported by a grant (325-4539-85/3) from the Bundesministe-
(Tib-Molbiol, Berlin) for rapid service in oligonucleotide synthesis;
rium für Gesundheit and a grant (E/B41G/1G309/1A403) from the
to Volker Thiel and John Ziebuhr (University of Würzburg) for pro-
Bundesamt für Wehrtechnik und Beschaffung. Studies conducted
viding human coronavirus 229E; to Georg Herrler (Tierärztliche
at the Institute of Medical Virology in Frankfurt were supported in
Hochschule, Hannover) for providing bovine coronavirus, avian
part by the Ministry of Science and Arts of the federal state of Hes-
infectious coronavirus, porcine transmissible gastroenteritis co-
sen, Germany.
ronavirus, and human coronavirus OC43; and to Michèle Bouloy
We are indebted to the medical staff of the hospital in Hanoi,
and Annette Martin for providing culture cells.
n engl j med 348;20
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
r e f e r e n c e s
Severe acute respiratory syndrome
low fever virus by real-time reverse tran-
al. Viruses and bacteria in the etiology of the
(SARS). Wkly Epidemiol Rec 2003;78:81-3.
scription-PCR. J Clin Microbiol 2002;40:
common cold. J Clin Microbiol 1998;36:
Acute respiratory syndrome China, Hong
Kong Special Administrative Region of Chi-
Felsenstein J. PHYLIP (Phylogeny Infer-
10. Cossart Y. TTV a common virus, but
na, and Viet Nam. Wkly Epidemiol Rec 2003;
ence Package), version 3.57c. Washington,
pathogenic? Lancet 1998;352:164.
D.C.: Department of Genetics, University of
11. Kew MC, Kassianides C. HGV: hepatitis
Tsang KW, Ho PL, Ooi GC, et al. A clus-
Washington, 2000. (Accessed April 22, 2003,
G virus or harmless G virus? Lancet 1996;
ter of cases of severe acute respiratory syn-
at http://evolution.genetics.washington. edu/
348:Suppl 2:sII-10.
drome in Hong Kong. N Engl J Med 2003;
12. Poutanen SM, Low DE, Henry B, et al.
Stephensen CB, Casebolt DB, Gango-
Identification of severe acute respiratory
Cumulative number of reported cases of
padhyay NN. Phylogenetic analysis of a
syndrome in Canada. N Engl J Med 2003;
severe acute respiratory syndrome (SARS).
highly conserved region of the polymerase
Geneva: World Health Organization, 2003.
gene from 11 coronaviruses and develop-
13. Cho KO, Hoet AE, Loerch SC, Wittum
(Accessed April 22, 2003 at http://www.
ment of a consensus polymerase chain reac-
TE, Saif LJ. Evaluation of concurrent shed-
tion assay. Virus Res 1999;60:181-9.
ding of bovine coronavirus via the respirato-
Drosten C, Göttig S, Schilling S, et al.
Günther S, Emmerich P, Laue T, et al.
ry tract and enteric route in feedlot cattle.
Rapid detection and quantification of RNA
Imported lassa fever in Germany: molecular
Am J Vet Res 2001;62:1436-41.
of Ebola and Marburg viruses, Lassa virus,
characterization of a new Lassa virus strain.
Copyright 2003 Massachusetts Medical Society.
Crimean-Congo hemorrhagic fever virus,
Emerg Infect Dis 2000;6:466-76.
Rift Valley fever virus, dengue virus, and yel-
Makela MJ, Puhakka T, Ruuskanen O, et
full text of all journal articles on the world wide web
Access to the complete text of the Journal on the Internet is free to all subscribers. To use this Web site, subscribers should go to
the Journal' s home page (http://www.nejm.org) and register by entering their names and subscriber numbers as they appear on
their mailing labels. After this one-time registration, subscribers can use their passwords to log on for electronic access to the
entire Journal from any computer that is connected to the Internet. Features include a library of all issues since January 1993 and
abstracts since January 1975, a full-text search capacity, and a personal archive for saving articles and search results of interest.
All articles can be printed in a format that is virtually identical to that of the typeset pages. Beginning six months after publication
the full text of all original articles and special articles is available free to nonsubscribers who have completed a brief registration.
Downloaded from www.nejm.org on June 28, 2003.
For personal use only. No other uses without permission. All rights reserved.
Source: http://www.batou.net/pdf_cursus/NEJM_34820.pdf
Comparison of olopatadine 0.6% nasal spray versusfluticasone propionate 50 g in the treatment of seasonalallergic rhinitis Michael A. Kaliner, M.D.,* William Storms, M.D.,# Stephen Tilles, M.D.,§ Sheldon Spector, M.D.,¶Ricardo Tan, M.D.,¶ Craig LaForce, M.D.,储 Bobby Q. Lanier, M.D.,** and Bradley Chipps, M.D.## The efficacy of nasal antihistamines (NAHs) for allergic rhinitis (AR) is comparable with or better than second-generation
Action against AIDS Aktionsbündnis gegen AIDS Indian Generics and Aids A Fact Finding Mission in the "Pharmacy of the Poor" Indische Generika und Aids Eine Erkundungsreise in der „Apotheke der Armen" Das Aktionsbündnis gegen AIDSDas Aktionsbündnis gegen AIDS will mit seiner Kampagne das Schweigen über HIV/Aids brechen und setzt sich ein für eine